

Collective trauma: A boy walks among some of the 3,000 flags placed in memory of the lives lost in the September 11, 2001 terrorist attacks. Jim Young/Reuters
![]()
09.11.2016
How the Pain of 9/11 Still Stays with a Generation

By Dr. Dana Rose Garfin
Research Scientist, Department of Psychology and Social Behavior
University of California, Irvine
The Sept. 11, 2001 (9/11) terrorist attacks were the worst acts of terrorism on American soil to date. Designed to instill panic and fear, the attacks were unprecedented in terms of their scope, magnitude and impact on the American psyche.
The vast majority (over 60 percent) of Americans watched these attacks occur live on television or saw them replayed over and over again in the days, weeks and years following the attacks.
As we reflect on the 15th anniversary of this tragic event, a question to consider is: How has this event impacted those individuals who are too young to remember a world before 9/11?
As an applied social psychologist, I study responses to natural and human-caused adversities that impact large segments of the population – also called “collective trauma.” My research group at the University of California, Irvine (UCI) has found that such exposures have compounding effects over the course of one’s lifespan. This is particularly relevant for children who have grown up in a post-9/11 society.
PTSD and Ground Zero
Many of the outcomes on which my team and I focus involve mental health, such as post-traumatic stress symptoms (PTS) and post-traumatic stress disorder (PTSD).
Post-traumatic stress symptoms include feeling the event is happening again (e.g., flashbacks, nightmares), avoiding situations that remind individuals of the event (e.g., public places, movies about an event), negative feelings and beliefs (e.g., the world is dangerous) or feeling “keyed up” (e.g., difficulty sleeping or concentrating).

Collective trauma is experienced by those who might not be near at the time of the event. Jim Young/Reuters
In order to meet diagnostic criteria for PTSD, an individual must have been directly exposed to a “traumatic event” (e.g., assault, violence, accidental injury). Direct exposure means that an individual (or their loved one) was at or very near the site of the event. It might be somewhat obvious that people directly exposed to a collective trauma like 9/11 might suffer from associated physical and mental health problems. What is less obvious is how people geographically distant from the epicenter or “Ground Zero” might have been impacted.
This is particularly relevant when considering the impact of 9/11 on children and youth across America: Many reside far from the location of the actual attacks and were too young to have experienced or seen the attacks as they occurred. The point is people can experience collective trauma solely through the media and report symptoms that resemble those typically associated with direct trauma exposure.
Impact on physical and mental health
The events of 9/11 ushered in a new era of media coverage of collective trauma, where terrorism and other forms of large-scale violence are transmitted into the daily lives of children and Americans families.
I have been exploring these issues with my collaborators Roxane Cohen Silver and E. Alison Holman. My colleagues surveyed a nationally representative sample of over 3,400 Americans shortly after 9/11 and then followed them for three years after the attacks.
In the weeks and months following the 9/11 attacks, media-based exposure was associated with psychological distress. This included acute stress (which is similar to PTS but must be experienced in the first month of exposure), post-traumatic stress and ongoing fears and worries about future acts of terrorism (in the months following the attacks).
These harmful effects persisted in the years following 9/11. For example, the team found measurable impact on the mental and physical health (such as increased risk of heart diseases) of the sample three years after the attacks. Importantly, those who responded with distress in the immediate aftermath were more likely to report subsequent problems as well.
These findings bear close resemblance to research led by psychologist William Schlenger, whose team found that Americans who reported watching more hours of 9/11 television in the immediate aftermath of 9/11 were more likely to report symptoms resembling PTSD. For example, those who reported watching four to seven hours were almost four times as likely to report such symptoms compared to those who watched less.
These findings were echoed in work conducted by Michael W. Otto, who also found that more hours of 9/11-related television watching was associated with higher post-traumatic stress symptoms in children under 10 in the first year following the attacks.
9/11’s impact on children
However, it is also the case that studies have found the number of children who reported longer-term distress symptoms to be relatively low. Among other factors, children whose parents had low coping abilities or themselves had learning disabilities tended to report higher distress.
For example, my collaborator Virginia Gil-Rivas, who studied American adolescents exposed to 9/11 only through the media, found that symptoms of post-traumatic distress decreased in most adolescents at the one-year mark. An important finding of her study was how parental coping abilities and parental availability to discuss the attacks made a difference.

What’s been the impact on children? Gary Hershorn/Reuters
Furthermore, children who had prior mental health problems or learning disabilities tended to be at higher risk for distress symptoms. That could be because children prone to anxiety in general experienced increased feelings of vulnerability.
Despite the number of studies that have followed children over the course of several years, no studies have comprehensively examined the long-term impact of 9/11 on children’s development and adjustment. That is because it is difficult to compare American children who lived through 9/11 with those who did not, since almost every American child was exposed to images of 9/11 at some point in time.
This limits the ability of researchers to examine how children’s lives might have changed over time.
However, some researchers believe that even media-based exposure to collective trauma could likely have a longer-term impact on the attitudes and beliefs of those who grew up in a post-9/11 world. It is possible, for example, that exposure to 9/11 and other acts of terrorism has led to fears of perceived threats, political intolerance, prejudice and xenophobia in some American children.
How 9/11 trauma impacts people today
Fifteen years later, a bigger question is: How does the collective trauma of 9/11 affect people today?
Over the past several years, my team and I have sought to address many of the issues that remained unanswered in the scientific literature after 9/11. We sought to replicate and extend the findings initially produced after 9/11 through an examination of responses to the 2013 Boston Marathon bombing, the worst act of terrorism in America since 9/11.
To this end, we surveyed 4,675 Americans. Our sample was demographically representative, meaning that our sample proportionally matched the U.S. Census data on key indicators such as ethnicity, income, gender and marital status.
This allowed us to make stronger inferences about how “Americans” responded. Within the first two to four weeks of the Boston Marathon bombings, we surveyed our sample about their direct and media-based exposure to the 2013 Boston Marathon bombing and their subsequent psychological responses.
Our study found that as media exposure (a sum of daily hours of Boston Marathon bombing-related television, radio, print, online news and social media coverage) increased, so did respondents’ acute stress symptoms. This was even after statistically accounting for other variables typically associated with distress responses (such as mental health).
People who reported more than three hours of media exposure had higher probability of reporting high acute stress symptoms than were people who were directly exposed to the bombing.
Then, last year, we sought to explore whether the accumulation of exposure to events like 9/11 and other collective trauma might influence responses to subsequent events like the Boston Marathon bombing.

A runner approaches the finish line during the 120th running of the Boston Marathon. Gretchen Ertl/Reuters
Once again, we used data from demographically representative samples of people who lived in the New York and Boston metropolitan areas. We assessed people who lived in the New York and Boston areas to facilitate a stronger comparison of direct and media-based exposure to 9/11 and the Boston Marathon bombing: people who lived in New York or Boston were more likely to meet criteria for “trauma exposure.”
This study had two primary, congruent findings. First, people who experienced greater numbers of direct exposure to prior collective trauma (e.g., 9/11, the Sandy Hook Elementary School shooting, Superstorm Sandy) reported higher acute stress symptoms after the Boston Marathon bombings.
Second, greater amounts of media-based live exposure (i.e., people watched or listened to the event as it occurred on live television, radio, or online streaming) to prior collective trauma were also associated with higher acute stress symptoms after the Boston Marathon bombing.
So greater direct and media-based exposure to prior collective trauma was linked with greater acute stress responses (e.g., anxiety, nightmares, trouble concentrating) after a subsequent event.
Stay informed, but limit exposure
Overall, our research indicates that the impact on children growing up post-9/11 likely extends well beyond the physical and mental health effects of exposure – be it direct or media-based. Each tragic incident that individuals witness, even if only through the media, likely has a cumulative effect.

People are resilient, but they need to be aware of the potential for distress. DVIDSHUB
Nevertheless, the positive finding is that most people are resilient in the face of tragedy. In the early years following 9/11, several studies examined how 9/11 impacted children nationally. Like adults, children exposed both directly and through the media tended to be resilient in the early years following the attacks and symptoms generally decreased over time.
Even so, being aware of the potential for distress through media exposure is important. Even small percentages can have large implications for our nation’s physical and mental health. For example, in the case of 9/11, 10 percent of a nationally-representative sample reporting post-traumatic stress represents 32,443,375 Americans with similar symptoms.
So, people should stay informed, but limit repeated exposure to disturbing images, which can elicit post-traumatic stress and lead to negative psychological and physical health outcomes.
Disaster Communications: Lessons from 9/11

By Dr. Thomas Terndrup (left) and Dr. Nicholas Kman (right)
Terndrup – Professor of Emergency Medicine
Kman – Associate Professor of Emergency Medicine
Ohio State University

The view from Brooklyn on September 11, 2001. Sara K. Schwittek/Reuters
“The hotel is being evacuated. Please return to your rooms and prepare to exit.” That was the first communication one of us, Dr. Terndrup, recalls receiving at a medical research meeting in the Brooklyn Marriott hotel that September morning.
Out on the street was pandemonium, Terndrup remembers. Just two miles from what would come to be called “Ground Zero,” people were running away from Manhattan. Members of our team – all medical professionals – split up to find ways to help. With a medic I had never met before, and whose name I didn’t ever learn, I walked across the Brooklyn Bridge, toward the World Trade Center site. Most people were heading the other way, of course.
The medic and I didn’t know quite what to do, though, because we didn’t know what was going on. We could see the smoke and ash covering much of the city skyline, as we headed in to help. Even the nonstop TV coverage didn’t give us many details we could use. Once we got to Manhattan, we got some useful information from police and other medics. But despite being in the heart of a major city with television cameras everywhere and thousands of emergency workers responding, it was challenging to get accurate, timely information.
What we and the other responders learned that day, under the pressure of a disaster of incredible scale, scope and urgency – not to mention the international media spotlight – went on to spark major changes in U.S. emergency response communication.
Setting up to respond

Makeshift clinics were set up in the area, including this one in Liberty Park. Reuters
Once over the bridge and into lower Manhattan, the medic and I found our way to an office building off Vesey and Church streets, where we joined several dozen doctors, nurses, paramedics, police, firefighters and others hoping to help. We set up a makeshift clinic, including securing four elevators to stay on the ground floor to serve as “treatment rooms.” Then we waited.
When someone said there was a group of exhausted firefighters in a nearby bank, a few people went over to help rinse out their smoke- and dust-filled eyes (the most common problem) and help them use nebulizers (acquired from a nearby pharmacy) to combat the effects of smoke inhalation.
Communications were primitive at best. Cellular service was completely gone. In the first few minutes after the planes hit the towers, New York City’s 9-1-1 call centers received 3,000 calls – throughout that day, more than 55,000 came in.
Thousands of law enforcement officers and firefighters were trying to connect by phone, radio and two-way pager. Devices and networks, not to mention personnel, were overloaded. Police radios were generally working, but the best information was often by word of mouth.
At our office-building clinic, the volunteers resorted to face-to-face communication, sending people to meet up with a group of responders gathering on the nearby Pace University campus and bring back what information they could. The main message rapidly went from bad to worse. It could be summed up as, “There’s nobody coming out of that alive.”
Planning to communicate
While obviously both of us hope nothing like that ever happens again, as emergency responders it’s our job to plan for the unthinkably disastrous. No matter what, responders need to be able to deliver messages to the public, talk to hospitals, and connect with each other.
Since 1999, New York City’s Office of Emergency Management, charged with coordinating all aspects of the response, had occupied permanent headquarters in Seven World Trade Center, on Greenwich Street, just north of the landmark twin towers. A vital communications link was the radio repeater system based on the ground floor of One World Trade Center, the north tower. The loss of those facilities – and key personnel working there – significantly hampered the response.
Today, it’s considered a bad idea to put an emergency operations center near places likely to be direct targets or at risk for collateral damage. When building a new emergency-response headquarters, New York City put it across the East River in downtown Brooklyn, far from all potential targets and landmarks in lower Manhattan.
Making the connections
But that distance can be a weakness if communications are reduced, as we were, to sending messengers on foot to have face-to-face conversations to relay information.
Even if radios and phones are working, they’re much less useful if responders can’t talk to each other. In 2001, the Fire Department of New York, the New York Police Department and the Port Authority Police all used different radio systems with different capabilities on different frequencies. Unable to connect with each other, neither the agencies nor the rescuers themselves could efficiently coordinate to help victims. This disconnection may also have prevented the evacuation of responders before the buildings fell.
If leaders are to be farther away and yet still act rapidly in an unfolding situation, they need more than one way to communicate with each other and with people directly on the scene. When one system gets cut off or stops working properly, there must be other options.
Constructing resilience
In our work with Ohio’s FEMA Urban Search and Rescue Team, Task Force 1, we have multiple communication methods. Mainly we use a national wireless network – which itself is designed to be resilient in emergencies, with redundant network connections and switching equipment and round-the-clock system monitoring. The company can also bring in portable cellular towers when regular cell towers are disabled, or to improve coverage in an area where existing service is overloaded.
We have wireless service for the bus that serves as our mobile operations center, and for cell phones and tablets issued to our task force leaders. The bus also has a Wi-Fi system that can connect additional devices.
If the cellular network is severely compromised by the disaster, we can use satellites. MSAT devices carry our voice traffic, and our data travels via portable BGAN terminals, which connect to laptop computers.
Our base of operations (BoO) at a disaster is equipped with a 1.8-meter VSAT satellite dish that can provide data and internet access for all the responders in the area. As further backup, we have portable radios and a repeater system.
What we communicate about

Medical personnel wait outside of St. Vincent’s Hospital, New York City, on September 11, 2001. Reuters
Another communications lesson from 9/11 comes from something that, tragically, didn’t happen. That day, New York hospitals called in all available staff, to be ready to receive large numbers of patients. They worried, as did we, in our makeshift clinic just north of the twin towers, that thousands of people would need lifesaving care all at the same time.
Yet there was no way to know which hospitals were full, which ones had operating rooms available or anything else about where to send patients, had they arrived in large numbers. Some hospitals likely would have been beyond overwhelmed, while others nearby might have had plenty of space and available doctors and nurses standing ready.
The lesson has spread across the country. Columbus, Ohio, where we work now, uses a system called “Real Time Activity Status,” which connects all the hospitals in our own Franklin County and three neighboring counties. It notifies ambulance dispatchers when their emergency rooms are too busy and need to divert patients to other hospitals. A similar system saved many lives after the 2013 Boston Marathon bombing.
By ensuring that – no matter what happens – we can communicate with each other, the emergency response community keeps the memory of 9/11 alive in our own way every single day.
How Building Design Changed after 9/11

By Dr. Shih-Ho Chao
Associate Professor of Structural Engineering and Applied Mechanics
University of Texas, Arlington

The new One World Trade Center building, made with high-performance concrete. John D. Morris
When buildings collapse killing hundreds – or thousands – of people, it’s a tragedy. It’s also an important engineering problem. The 1995 collapse of the Alfred P. Murrah Federal Building in Oklahoma City and the World Trade Center towers in 2001 spawned many vows to never let anything like those events happen again. For structural engineers like me, that meant figuring out what happened, and doing extensive research on how to improve buildings’ ability to withstand a terrorist attack.
The attack on the Murrah building taught us that a building could experience what is called “progressive collapse,” even if only a few columns are damaged. The building was nine stories tall, made of reinforced concrete. The explosion in a cargo truck in front of the building on April 19, 1995, weakened key parts of the building but did not level the whole structure.
Only a few columns failed because of the explosion, but as they collapsed, the undamaged columns were left trying to hold up the building on their own. Not all of them were able to handle the additional load; about half of the building collapsed. Though a large portion of the building remained standing, 268 people died in the areas directly affected by the bomb, and in those nearby areas that could no longer support themselves. (A month after the attack, the rest of the building was intentionally demolished; the site is now a memorial to the victims.)

The progressive collapse of the North Tower. Jason Valdina/flickr
A similar phenomenon was behind the collapse of the World Trade Center towers on September 11, 2001, killing nearly 3,000 people. When exposed to the high temperatures created by burning airplane fuel, steel columns in both towers lost strength, putting too much load on other structural supports.
Until those attacks, most buildings had been built with defenses against total collapse, but progressive collapse was poorly understood, and rarely seen. Since 2001, we now understand progressive collapse is a key threat. And we’ve identified two major ways to reduce its likelihood of happening and its severity if it does: improving structural design to better resist explosions and strengthening construction materials themselves.
Borrowing from earthquake protection
Research has found ways to keep columns and beams strong even when they are stressed and bent. This property is called ductility, and higher ductility could reduce the chance of progressive collapse. It’s a common concern when building in earthquake-prone areas.
In fact, for years building codes from the American Society of Civil Engineers, the American Institute of Steel Construction and the American Concrete Institute have required structural supports to be designed with high enough ductility to withstand a major earthquake so rare its probability of happening is once every 2,000 years. These requirements should prevent collapse when a massive earthquake happens. But it’s not enough to just adopt those codes and expect they will also reduce or prevent damage from terrorist attacks: Underground earthquakes affect buildings very differently from how nearby explosions do.
Another key element structural engineers must consider is redundancy: how to design and build multiple reinforcements for key beams and columns so the loss of, say, an exterior column due to an explosion won’t lead to total collapse of the entire structure. Few standards exist for redundancy to improve blast resistance, but the National Institute for Building Sciences does have some design guidelines.
Making concrete stronger
The materials that buildings are made of also matter. The steel columns in the World Trade Center towers lost strength rapidly when the fire reached 400 degrees Fahrenheit. Concrete heated to that temperature, though, doesn’t undergo significant physical or chemical changes; it maintains most of its mechanical properties. In other words, concrete is virtually fireproof.
The new One World Trade Center building takes advantage of this. At its core are massive three-foot-thick reinforced concrete walls that run the full height of the building. In addition to containing large amounts of specially designed reinforcing bars, these walls are made of high-strength concrete.
An explosion generates very high pressure – how much depends on how big the blast itself is, and how close it is to the structure. That leads to intense stress in the concrete, which can be crushed if it is not strong enough.
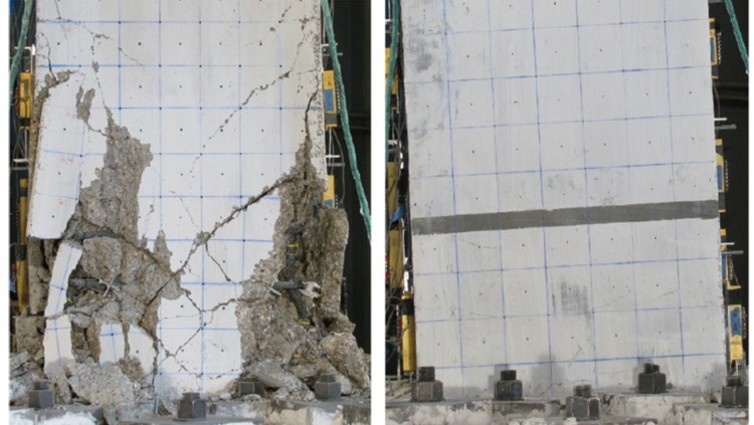
At left, standard reinforced concrete; at right, ultra-high-performance fiber-reinforced concrete, under similar severe earthquake loadings. Shih-Ho Chao
Regular concrete can withstand 3,000 to 6,000 pounds of compression pressure per square inch (psi); the concrete used for One World Trade Center has a compressive strength of 12,000 psi. Using materials science to more densely pack particles, concrete’s strength has been increased up to 30,000 psi.
Improving reinforcement

High-strength steel fibers like this are mixed into concrete to make it even stronger and tougher. Shih-Ho Chao
While traditional reinforced concrete involves embedding a framework of steel bars inside a concrete structural element, recent years have brought further advancement. To enhance concrete’s toughness and blast resistance, high-strength needle-like steel microfibers are mixed into the concrete. Millions of these bond with the concrete and prevent the spreading of any cracks that occur because of an explosion or other extreme force.
This mix of steel and concrete is superstrong and very ductile. Research has shown that this material, called ultra-high-performance fiber-reinforced concrete, is extremely resistant to blast damage. As a result, we can expect future designers and builders to use this material to further harden their buildings against attack. It’s just one way we are contributing to the efforts to prevent these sorts of tragedies from happening in the future.
Flashbulb Memories of Dramatic Events Aren’t as Accurate as Believed

By Dr. Jennifer Talarico
Associate Professor of Psychology
Lafayette College

Flashbulb memories of 9/11 are more vivid than ordinary memories, but no more accurate. Shannon Stapleton
Where were you on Sept. 11 when you first heard that a plane had hit the North Tower of the World Trade Center?
Many of us may have vivid memories of that day, recalling where we were and what we were doing when we first learned of the attack, perhaps even remembering seemingly irrelevant details. Chances are, that memory isn’t as accurate as you think it is.
This is called a flashbulb memory. Researchers coined the term in the 1970s as a metaphor for capturing an entire scene in one moment, from the most important to the most mundane details, and then being able to hold on to that memory indefinitely as if you had a photographic record of it.
Flashbulb memories have intrigued memory researchers like me for a long time. We know that they are a type of autobiographical memory – memories of personally experienced events. Like other autobiographical memories, we think we remember them accurately. In reality, we often don’t.
While we know that flashbulb memories aren’t perfect records, for a long time no one knew if these memories were more accurate than ordinary autobiographical memories. Since flashbulb memories are often formed after sudden, dramatic events, it’s hard to create experiments to test this.
I was a graduate student at Duke University on Sept. 11, 2001. My adviser, David Rubin, and I instantly recognized the opportunity to conduct a study of flashbulb memories in response to the event.
On Sept. 12, we asked our undergraduates about their memories of how they learned about the terrorist attacks, as well as an ordinary autobiographical memory from the preceding weekend. In the months afterward, we were able to follow up with our undergrads to see if and how their memories changed.
You think you remember it exactly, but you don’t
While the term “flashbulb memory” was introduced in 1977, the phenomenon was known to researchers well before then. In fact, in 1899 psychologist F. W. Colegrove recorded vivid and detailed memories from people about when they learned of President Lincoln’s assassination.
For a long time, researchers argued that flashbulb memories really were a complete and accurate snapshot of events.
Ulric Neisser, a pioneering cognitive psychologist, drew on a flashbulb memory of his own to suggest that this wasn’t the case in 1982. Here is how he described his memory of learning about the attack on Pearl Harbor:
“I recall sitting in the living room of our house – we only lived in that house for one year, but I remember it well – listening to a baseball game on the radio. The game was interrupted by an announcement of the attack, and I rushed upstairs to tell my mother.”
Years later, after reading scientific research on flashbulb memories, Neisser realized that this memory had to be wrong. Pearl Harbor was attacked on Dec. 7, and there is no baseball on the radio in December.
This realization led him to explore the accuracy of flashbulb memories.

People’s memories of the Challenger disaster changed over time. In this photo the Challenger crew takes a break during countdown training at NASA’s Kennedy Space Center on January 9, 1986. Reuters/NASA/Handout
In 1986, Neisser and his collaborator Nicole Harsch asked a group of undergraduates to recall how they learned of the Challenger space shuttle disaster the morning after it happened. Much like earlier reports, they found that almost all of the students had detailed memories of “exactly” where they were and what they were doing when they found out about the explosion.
Neisser and Harsch did something that other researchers hadn’t done before. They asked participants to recall the same event a few years later. They found that although everyone still had vivid and complete memories, some of the memories had changed quite remarkably. In fact, 25 percent of participants reported different memories altogether, such as first describing having learned from a fellow student in class, and years later saying they saw it on a TV news bulletin with their roommate.
This meant that the vividness and confidence that participants had shown were not related to the actual accuracy of their memories.
And the errors that flashbulb memories develops are not random. Our emotions and sense of belonging to a group can color them. For instance, Neisser was probably listening to a football game on the radio when he heard about Pearl Harbor. He argued that the switch from football to baseball served to emphasize his personal connection to the “national pastime” at a time when that nation, to which he was an immigrant, had been attacked.
And a 2005 study found that Danes remember the day when Denmark surrendered to Germany in World War II as being colder, cloudier, windier and rainier than it truly was and the day when Denmark was liberated from Germany as being warmer, sunnier, less windy and less rainy than it truly was.
While these studies demonstrate that flashbulb memories aren’t completely accurate, they don’t test whether flashbulb memories are more accurate than memories of everyday events.
That was the question that my colleague and I sought to address in the wake of the Sept. 11 attacks.
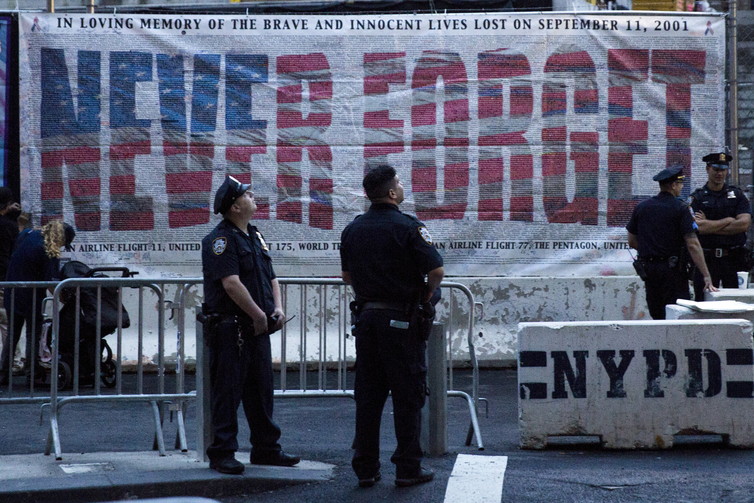
New York police officers gather before a ceremony marking the 14th anniversary of the 9/11 attacks, at the National September 11 Memorial and Museum in Lower Manhattan in New York on September 11, 2015. Andrew Kelly/Reuters
Flashbulb memories vs. ordinary memories
On Sept. 12, David Rubin and I asked a group of 54 undergraduates questions about how they learned about the attacks. We asked questions about the memory like, “How did you learn the news?” “Where were you?” “What were you doing?” and “Who were you with?” We also asked questions about the feeling of remembering like, “How clearly can you see this event in your mind’s eye?” and “How strongly do you believe that the event actually happened in the way that you are remembering it?”
We also asked participants the same questions about another memorable event from the weekend before the attacks. By doing so, we could directly compare how flashbulb memories and ordinary memories of life events change over time.
We then asked subgroups of our participants the same questions either one week, one month, or seven months later. By recruiting subgroups at each time point, each person only told us about their memories twice, but we were able to observe how memories changed over three distinct time points.
Flashbulb and ordinary autobiographical memories were very consistent over the course of one week. By one month and certainly by seven months, both memories showed fewer consistent details between the two reports. The rate of that forgetting was the same for both types of memories.
We also found that errors, like the introduction of new or contradictory information, were introduced at about the same rate in both types of memories.
So what is the difference between flashbulb memories and autobiographical memories? Our beliefs about those memories.
People believed that their flashbulb memories were more accurate than the ordinary memory we asked them to recount. They felt that they remembered the flashbulb memory more vividly as well. And it’s this difference in perception that makes flashbulb memories so remarkable.
We believe flashbulb memories are accurate
So why do we believe that these flashbulb memories are more accurate than other memories?
For our sample of American students, the attacks of 9/11 were highly emotional and dominated not just national discourse but also much of private conversation for days and weeks later. These processes serve to enhance the vividness of our memories and our subjective confidence in those recollections.
Furthermore, by virtue of having these long-lasting and detailed memories of significant events, we can demonstrate and reinforce our membership in these important social groups. In other words, community exhortations to “never forget” serve to maintain memories not just collectively, but individually.