
By Dr. John Frith
Phthisis, Consumption, and the White Plague
Overview
A phthitic soldier is to his roommates what a glandered horse is to its stablemates.[1]
Jean Antoine Villemin, French Army surgeon, 1865
Tuberculosis is an infection with Mycobacterium tuberculosis which can occur in any organ of the body but is most well known in the lung. It has been a scourge throughout known history and may have killed more persons than any other microbial pathogen. [2] Paleopathological evidence dates back to 8000 BCE and evidence of bony tuberculosis has been found dating from the Neolithic period in 5800 BCE and in Egyptian mummies dating to 2400 BCE. [1, 3]
Tuberculosis was also known as phthisis and consumption from Hippocrates through to the 18th century [1], the white death [4] and the great white plague [5] during the 19th century, and other names which evoked the despair and horror of the disease such as the robber of youth [6], the Captain of all these men of Death [7], the graveyard cough [8], and the King’s-Evill [4]. During the 18th and 19th centuries tuberculosis was epidemic in Europe and caused millions of deaths, particularly in the poorer classes of society. Tuberculosis declined after the late 19th century but remained a major public health issue as it still is today. [9]
Tuberculosis is an important disease for the military. During both World War I and World War II in the US Army, tuberculosis was the leading cause of discharge. [10] Annual incidence of tuberculosis in the military of Western countries is very low, however in the last several decades microepidemics have occurred in small close knit units on US and British Naval warships and land based units deployed overseas. Living and working in close quarters and overseas deployment to tuberculosis-endemic areas of the world such as Afghanistan, Iraq and South-East Asia remain significant risk factors for tuberculosis infection in military personnel, particularly multidrug resistant tuberculosis. . [11, 12]
Descriptions of Tuberculosis from Antiquity
The legal text written in cuneiform on a stone pillar by Hammurabi, a Babylonian king, in the 2nd millennium BCE mentions a chronic lung disease which may have been tuberculosis, and a “wasting disease” was described in one of the earliest medical works, the Chinese Huang Ti Nei-Ching in the third millennium BCE. Homer’s epic poem Odyssey from the 8th century BCE refers to “grievous consumption which took the soul from the body and caused a person to “lie in sickness …. a long time wasting away””. [1, 9, 13]
Hippocrates in Book 1, Of the Epidemics (410-400 BCE) described a disease of “weakness of the lung” with fever and cough which he refers to as phthisis (Gr. phthiein = to waste away). Phthisis was described as the commonest disease of the period and usually as being fatal. [1, 14]
Early in the beginning of spring, and through the summer, and towards winter, many of those who had been long gradually declining, took to bed with symptoms of phthisis; …. Many, and, in fact, most of them died, and of those confined to bed, I do not know of a single individual survived for any considerable time, …. Consumption was the most considerable of the diseases which then prevailed, and the only one which proved fatal to many persons. Most of them were affected by these diseases in the following manner; fevers accompanied with rigors, … constant sweats, … extremities very cold, and warmed with difficulty; bowels disordered, with bilious, scanty, unmixed, thin, pungent, and frequent dejections. The urine was thin, colourless, unconcocted, or thick, with a deficient sediment. Sputa small, dense, concocted, but brought up rarely and with difficulty; and in those who encountered the most violent symptoms there was no concoction at all, but they continued throughout spitting crude matters.[14]
Hippocrates recognised the predilection of the disease for young adults, “Phthisis makes its attacks chiefly between the age of eighteen and thirty five”. [14] He also considered that pulmonary phthisis was a hereditary disease rather than an infectious one as it so commonly occurred throughout a whole family. [1, 15]
Aretaeus of Cappadocia in the 2nd century CE in his work De causis et signis diuturnorum morborum described phthisis with wasting, coughing of blood and the formation of empyema [1, 4, 16] and wrote:
If from an abscess in the lung or a settled cough or spitting of blood, pus should develop within and the patient should spit it out, the disease is called pyë and phthisis. But if the chest or a rib suppurates and pus comes out through the lungs it is called empyë. If after this, the lung, consumed by the passage of the pus, has an abscess, it is called phthoë.[16]
Claudius Galen of Pergamum, a Greek physician to the Roman Emperor Marcus Aurelius in 174 CE, described phthisis with fever, sweating and coughing of blood stained sputum, and found tubercles in phthitic lungs that he called phûma. He considered it to be infectious and warned against close contact with people with the disease. [9, 16]
Early Historical Treatments
In the Hippocrates’ era patients were nursed in temples and treated with plentiful and good food, milk, particularly asses’ milk (it was thought asses were not prone to phthisis), and exercise. Galen and other physicians of his time recommended fresh air, milk, particularly human breast milk, eating wolf livers, drinking elephant urine, and sea voyages to regions with gentle favourable winds such as Egypt and Libya. Bloodletting was often done as it was for many diseases. [1, 2, 8, 9, 16] Aretaeus of Cappadocia recommended those “weak in the lungs” have a prolonged sojourn in the blessed cypress groves at Apollo’s temple in Aquinum in Aratolia where the Sun God himself would heal them. [4] Pliny the Elder (23-79 CE) mentioned inhalation of stringent smoke and licking the limestone from Assos on the Troad coast; Pedacius Dioscorides, a Greek army surgeon in the service of Nero (54-68 CE) who wrote Materia Medica, recommended “warming drugs” such as animal fats; and Tertullian (160-225 CE) recommended butter boiled with honey. [16, 17]
Renaissance to the 19th Century

In 1679 Sylvius de la Boë, an Amsterdam physician, in his work Opera Medica, was probably the first to use the term tubercles in phthisis of the lung which he called tubercula glandulosa, “glandulous tubercles”, and described their progression to abscesses, ulcers, and empyema. In addition, Sylvius described the association between phthisis and a disease of the lymph glands of the neck called scrofula. [1, 13, 18]
Richard Morton, an English physician and physician to King James II, in his 1689 work Phthisiologia described the pathology of pulmonary and other forms of phthisis, tubercles of the lung, and scrofula. Both Sylvius and Morton considered phthisis was hereditary but Morton also considered it may be transmissible by intimate contact. [1, 18] Morton described the severity of the disease in young people, “the Consumption of Young Men, that are in the Flower of their Age”. [18]
In 1690 John Bunyan, British author of Pilgrim’s Progress, in his work The Life and Death of Mr. Badman referred to consumption as the Captain of all these men of Death: “He parts from his wife – diseases attack him under captain consumption, he rots away, and dies in sinful security … Yet the captain of all these men of death that came against him to take him away, was the consumption, for it was that that brought him down to the grave.”[7]
In 1702 Jean-Jacques Manget, a Genevan physician, observed at a post-mortem multiple small phthitic nodules in the lungs and organs which resembled millet seeds, later called “miliary tuberculosis”. [1, 5] In 1793 Matthew Baille, a Scottish pathologist who himself died from tuberculosis, described the caseous (“cheese-like”) appearance of phthitic abscesses. [4] In 1803 Gaspard-Laurent Bayle of Vernet described the tubercle and its association with pulmonary and other forms of phthisis which he published in his 1810 work Reserches sur la phthisie pulmonaire. [17, 18]
The term consumption was used as a lay term for phthisis in the 17th and 18th centuries, and both terms were used until the mid-19th century when the term tuberculosis was coined by Johann Lukas Schönlein and later used by Hermann Brehmer, Jean Antoine Villemin and Robert Koch. [1, 15]
René Théophile Hyacinthe Laennec
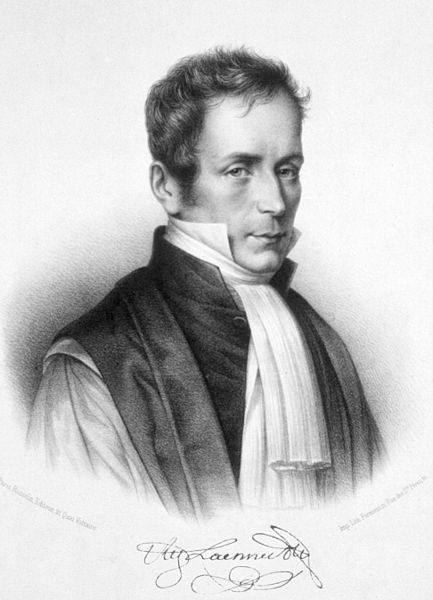
René Théophile Hyacinthe Laennec (1781-1826) was a renowned French physician and medical researcher. He began his medical studies in Nantes, and then later at the École Pratique in Paris where he studied cadaver dissection in Guillame Dupuytrens’ laboratory. Laennec distinguished himself as a student, winning prizes in both medicine and surgery in 1801, and in 1802 he published his first paper on rheumatic fever and mitral stenosis. Later he served as editor of the Journal de Médecine. Laennec became known for his description of the tawny yellow nodules of micronodular cirrhosis of the liver (from Gr “kirrhos” = tawny yellow), now known as Laennec’s cirrhosis. [19, 20]
In 1816 Laennec invented the stethoscope while working at the L’hôpital Necker in Paris, initially by rolling up his notebook, then later by constructing a hollow wooden cylinder. [4, 19, 20]
I therefore took a paper notebook, rolled it up tightly, applied one end to the pericardiac region and listened at the other. I was surprised as I was pleased to hear the heart beat much more clearly and distinctly.[4]
Laennec originally called his invention le Cylindre, but later called it a stethoscope, and called his auscultation method l’auscultation médiate (“mediate auscultation” – hearing carefully with the aided ear), or stethoscopy. Using a stethoscope helped preserve the modesty of female patients rather than having to have one’s ear on the patient’s chest or breast. Laennec’s stethoscope was a revolutionary advance in clinical medicine enabling for the first time an accurate description of normal function and in diseases of the heart and lungs. In 1818 he presented his findings and research on stethoscopy of the chest to the Académie des sciences in Paris and in 1819 published them in his work De l’auscultation mediate ou Traité du Diagnostic des Maladies des Poumon et du Coeur (On Mediate Auscultation or Treatise on the Diagnosis of the Diseases of the Lungs and Heart). [15, 19, 20]
Laennec wrote an accurate and reliable description of many diseases of the chest such as bronchiectasis, pneumonia, pleurisy, and emphysema, as well as tuberculosis. He used his stethoscope to listen to the chests of tuberculous patients, identifying the presence of consolidation, pleurisy, and pulmonary cavitation. Correlating his patient examination with his dissection findings, Laennec described pulmonary and extra-pulmonary tubercles in detail and showed that they were the first phase of phthisis. He described how they first appeared in the lung in their “miliary” (“millet seed-like”) form, progressing to larger tubercles containing “cheese-like” (“caseous”) material, their breakdown into pus, and eventually forming cavities and empyema. He also described extra-pulmonary phthitic tubercles in the intestines, liver, meninges and other organs, and tuberculous infection in vertebrae which caused vertebral collapse and spinal cord paralysis that had been described by Sir Percivall Pott, a British surgeon, in 1779, known as Pott’s disease. [4, 15, 17, 19, 20]
Laennec examined his patients according to the four pillars of French clinical method – inspection, palpation, percussion, and auscultation. He was a skilled dissector, relating findings at post-mortem to the patient’s symptoms in life, and was hailed as “the greatest of teachers on tuberculosis”. [4, 9, 17, 19] He was the originator of the terms “auscultation” (“listening carefully”), “rhonchus” ( a “whistling” or “snoring” sound), “pectoriloquy” (“the chest speaks”), “egophony” (“resonance”), and “râle” (a “rattling” sound) of which there were five types including “crépitation” ( a “moist rattling”). Laennec died from tuberculosis in 1826. [19, 20, 21]
Scrofula – “the King’s-Evill”
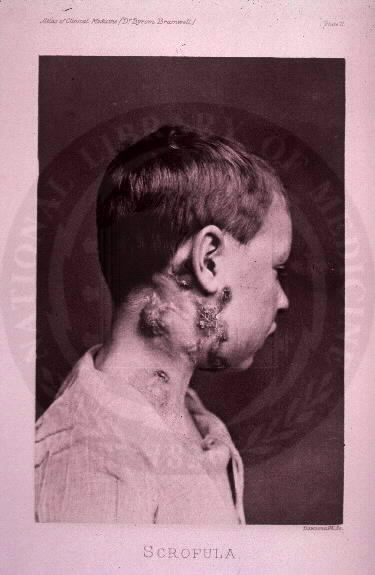
Scrofula is tuberculosis of the lymph glands of the neck with eventual ulceration and suppuration. Aristotle (384-322 BCE) and Cassius Felix (447 CE) were probably the first to describe scrofula. [1, 22] Scrofula was also known in the 17th century as “the King’s-Evill” because it was believed it could be cured by the King’s touch. Richard Wiseman, who served as a ship’s surgeon for the Dutch navy and later as a surgeon for King Charles’ I army, wrote on the King’s evil and its cure by the King in 1672 in his Treatise of the King’s-Evill in the fourth book of his Chirurgical Treatises. It was not known then however that scrofula was related to phthisis or consumption. [18]
The belief that disease could be cured by a king’s touch has its origins with Clovis of France (487-511), and later other European monarchs such as Robert the Pious, Edward the Confessor and Philip I of France. [17, 22, 23] The cure of scrofula by the King’s touch was common after the 13th century and performed by English and French monarchs such as King Charles II, who during his 25 year reign touched 92,102 subjects. [4, 9] Shakespeare in Macbeth, Act IV, Scene 3, refers to King Edward curing a “wretched crew of souls” of scrofula:
” … strangely-visited people,
All swoln and ulcerous, pitiful to the eye,
The mere despair of surgery, he cures;
Hanging a golden stamp about their necks,
Put on with holy prayers.; and ’tis spoken,
To the succeeding royalty he leaves
The healing benediction … ” [5]
Sylvius de la Boë, Richard Morton and René Laennec had all recognised that scrofula often occurred in association with pulmonary phthisis, however the fact the two diseases had the one cause was not known until the 19th century. [1]
The Epidemic of the 18th and 19th Centuries and the Romantic Image of Tuberculosis

By Laennec’s era, tuberculosis had become epidemic in Europe where annual mortality rates were between 800 and 1,000 per 100,000 per year. [2] Between 1851 and 1910 in England and Wales four million died from tuberculosis, more than one third of those aged 15 to 34 and half of those aged 20 to 24 died [9], and tuberculosis was called the robber of youth. [6]
In that time it also became known as the great white plague and the white death [4, 5, 24], called “white” because of the extreme anaemic pallor of those affected [4, 25]. The term white plague was used by Oliver Wendall Holmes, an American physician and writer, in 1861 in comparing the enormity of the epidemic to other severe plagues of the time. [26] Dormandy (1999) states that the term “white” may also have referred to its association with youth, innocence and even holiness. [4] Consumptive patients took on the appearance of a thin, pale, melancholy, almost delicate spirit. The wan and pallid facies of the victim was thought to be attractive and Dormandy states it gave women a “terrible beauty” [4].
The disease became romanticised in society by poets such as John Keats, Percy Bysshe Shelley, and George Lord Byron, and writers such as Edgar Allan Poe, Robert Louis Stevenson and Emily Brontë, many of whom themselves died from the disease. [2, 4, 27, 28] Byrne (2011) refers to the romantic poetry of Keats and Shelley which “sought to find beauty in the horror and melancholy of consumption”. Such poetry of the time was sometimes called “graveyard poetry”. Byron once remarked to his friend, Lord Sligo, “I should like, I think, to die of consumption.” When Lord Sligo asked why, Byron replied, “Because then all the women would say ‘See that poor Byron – how interesting he looks in dying.’” [28]
John Keats wrote in 1819, “Youth grows pale, and spectre thin, and dies.” [27] Keats died from tuberculosis in 1821 aged only 26 years. On a winter evening in 1818 when Keats was returning to his home in Hampstead Heath from London, he felt ill and immediately went to bed. He suddenly coughed blood onto his pillow and said to his friend John Arbuthnot Brown,
I know the colour of that blood. It is arterial blood, I cannot be deceived by its colour. It is my death warrant. I must die.[4, 5]
Edgar Allan Poe described his young wife, Virginia, who had tuberculosis as being ‘delicately, morbidly angelic’. In 1842 while they were having dinner, Virginia had a sudden coughing fit and haemoptysis and Poe remarked :
Suddenly she stopped, clutched her throat and a wave of crimson blood ran down her breast … It rendered her even more ethereal.[27]
Emily Brontë described the tuberculous heroine in Wuthering Heights as “rather thin, but young and fresh complexioned and her eyes sparkled like diamonds”. Emily, her four sisters, and her brother Branwell died in young adulthood from tuberculosis, and their mother also died of tuberculosis. [2, 4]
The imagery of the consumptive was also used by the writers of popular fiction of the 19th century who began the literary tradition of vampirism to describe vampires and their victims. Consequently it was sometimes thought, especially in areas of the world where such folklore abound such as New England in America and Yorkshire in northern Britain, that people seen to be suffering from what were actually symptoms of tuberculosis, the wasting and extreme pallor, were victims of vampires or were vampires themselves. [28].
There were certain social conditions that were intimately associated with the disease, linked to the industrial revolution at the time – poverty, malnutrition, and overcrowding. Conditions for the working classes were extremely poor. [8] In 1838 and 1839 in England between a quarter and a third of tradesmen and labourers died from tuberculosis compared to a sixth of “gentlemen”. [5]
The disease picked out and killed a few Princes and it carried off more than one bejewelled, tender-hearted courtesan; but it slaughtered the poor by the million.[4]
Wealthy tuberculosis sufferers could afford to travel in search of sunny and mild climates or seek refuge in mountain sanatoria, whereas poorer people had to look after their own ill consumptive family in dark, unventilated, closed rooms, sealing their own fate to die of the same disease a few years later. [4, 27]
The 19th Century Debate about the Pathology and Transmission of Phthisis
From the beginning of the 19th century physicians debated in earnest two important questions about the pathological foundations of phthisis – firstly whether it was infectious, hereditary, or cancer, and secondly, whether scrofula, tubercles, and phthisis were separate disease entities or manifestations of the one disease.
The most prominent proponents of a single entity were René Laennec and the Viennese pathologist Carl von Rokitansky. In contrast, Giovanna Battista Morgagni of Padua, and German physicians Rudolf Virchov and Johann Lukas Schönlein believed the diseases were separate entities. [1, 3] This question wasn’t settled until Robert Koch discovered in 1882 the Tubercle bacillus and that it was responsible for all forms of the disease.
By the 18th century many Italian physicians had come to believe that phthisis was infectious, although many British and American physicians at the time did not, and avoided doing autopsies on patients who had died from phthisis to protect themselves and their students. [1, 3, 5, 29] Many others however still thought phthisis to be hereditary or due to constitutional weakness. [2, 3] Another school of thought was that phthisis was related to zymes, chemicals that themselves did not cause diseases but acted as catalysts in causing decay within the body and could cause zymotic fevers. [9]
The 19th century saw several major breakthroughs in tuberculosis research that elucidated the infectious nature of the disease culminating in Robert Koch’s discovery of the bacteria. In 1843 Philipp Friedrich Hermann Klencke, a German physician, successfully inoculated rabbits with material from a tubercle although he believed the disease to be cancer. In 1844 Friedrich Gustav Jakob Henle, a German pathologist, postulated that phthisis was infectious. [1, 29]
The first breakthrough was in 1865 by Jean Antoine Villemin, a French military surgeon at the Army Medical School at Val-de Grâce. Villemin had observed that soldiers stationed for long times in barracks were more likely to have phthisis than soldiers in the field, and healthy army recruits from the country often became consumptive within a year or two of taking up their posts. He showed by controlled experiments that phthisis from humans, or tuberculosis as he also called it in his work Cause et nature de la tuberculose: son inoculation de l’homme au lapin, could be transmitted to rabbits demonstrating that the disease was infectious. Villemin thought that phthisis was similar to glanders, an infectious disease in horses. [1, 2, 4, 5, 17]
Koch’s discovery in 1882 of the bacillus that caused tuberculosis provided more evidence that the disease was infectious. In his acceptance of his Nobel Prize in 1905 he alluded to the work of his colleague and a fellow bacteriologist, Carl Flügge, that bacilli in droplets from a cough could possibly transmit infection. However it wasn’t until the mid-20th century that it was conclusively shown that tuberculosis was transmitted by the inhalation of contaminated air droplets. [30]
The Term “Tuberculosis”

Johann Lukas Schönlein, a German physician, in 1834 used the term tuberculosis in describing disease with tubercles, but did not use the term in relation to scrofula or phthisis. [1, 5, 15] In 1853 Hermann Brehmer, a medical graduate of the University of Berlin, used the term tuberculosis of the lungs in his doctoral thesis titled De legibus ad initium atque progressum tuberculosis pulmonum spectantibus, “On the Laws concerning the Beginning and Progress of Tuberculosis of the Lungs”, in which he also referred to tuberculosis being curable in its early stages. [29, 31] It appears that after this time the term tuberculosis supplanted phthisis, although consumption still remained as the lay term for the disease. Villemin used the term tuberculose in 1865 and in 1882 Robert Koch used the term tuberkulose, translated to English as tuberculosis, describing his discovery of the bacterium he called Tubercle bacillus, after which the disease was known as either tuberculosis or TB. [1, 3, 15, 32]
Robert Koch’s discovery paved the way for the development of the Pirquet and Mantoux tuberculin skin tests, Albert Calmette and Camille Guérin’s BCG vaccine, Selman Waksman’s streptomycin and other anti-tuberculous drugs. Tuberculosis is still a major public health problem today, in 2011, 8.7 million people were infected with tuberculosis with 1.4 million deaths, and mortality from tuberculosis has increased in recent decades with the emergence of HIV and of multi-drug resistant tuberculosis.
The Sanatoria and the Discoveries of the Tubercle Bacillus
If the importance of a disease for mankind is measured by the number of fatalities it causes, then tuberculosis must be considered much more important than those most feared infectious diseases, plague, cholera and the like. One in seven of all human beings dies from tuberculosis.”[1]
Robert Koch, in his address to the Berlin Physiological Society, 24th March 1882
Overview
Tuberculosis was epidemic in Europe and America in the 18th and 19th centuries, and by the mid 18th century in London and Hamburg, the mortality rates were as high as 1000 per 100,000 per year.2 The disease had a predilection for young people and was called the robberof youth3, and also for the poorer classes, who were disadvantaged by malnutrition, overcrowding and poor living and working conditions and who died by the millions over those two centuries.[4, 5]
The ravages of the disease spurred many scientists to find the cause and the cure. Sanatoria were developed in the mid 19th century where patients lived in open alpine or seaside air with good and ample food, but they were not effective at curing the disease and most still died from it.2, 6 Scientists and physicians also argued whether phthisis, scrofula and tubercular disease were separate entities or the one disease, and whether they were hereditary, cancer or infectious diseases. In 1865 Jean Antoine Villemin, a French military surgeon, showed by experiments in animals that phthisis was infectious. [2, 5, 6]. The second major breakthrough was the discovery in 1882 by Hermann Heinrich Robert Koch of the cause of tuberculosis – a bacillus he called Tubercle bacillus and which was later renamed Mycobacterium tuberculosis.[2, 6, 7]
Robert Koch’s Discovery of the Tubercle Bacillus in 1882
In 1882 Robert Koch, a German physician and one of the founders of bacteriology, discovered the bacillus that caused tuberculosis. Koch used material from cases of pulmonary, extra-pulmonary and meningeal tubercular disease as well as cases of scrofula. For staining Koch used methylene-blue in a solution of caustic potash. Culture of the bacteria was difficult, he eventually used a medium of coagulated bovine serum developed by John Tyndall, a British microbiologist. Koch then successfully inoculated bacteria from the culture to infect laboratory animals, thus fulfilling the postulates of infectious disease developed by his mentor from Göttingen, Friedrich Gustav Jakob Henle, and which he and Henle later modified to become the Henle-Koch postulates. Koch used his technique to demonstrate the presence of the bacillus in all forms of human and animal tuberculosis proving unequivocally not only that the bacillus was the cause, but the many different forms of tuberculosis were manifestations of the one disease entity.[2, 6, 7, 8, 9, 10]
Koch delivered his findings in a lecture to the Berlin Physiological Society at the Charité Hospital in Berlin on 24th March 1882 under the title Die Ätiologie derTuberkulose, “The Aetiology of Tuberculosis”.[1,6] The audience of Koch’s lecture listened in silence and awe and admiration to what must have been an extraordinarily enlightening presentation, afterwards the audience rose to look at Koch’s cultures and microscope slides of the bacillus. Paul Ehrlich, then assistant bacteriologist to Professor Friedrich von Frerichs at the Charité Hospital, Berlin, and who later discovered Salvarsan and became the founder of immunology and chemotherapeutics, was present at the lecture and remarked, “I hold that evening to be the most important experience of my scientific life.”[11]
On 10 April 1882 Koch published his lecture in the Berliner Medicinische Wochenschrift, and sent a copy to John Tyndall who in turn published Koch’s essential findings in a letter to The Times on 22 April 1882. The letter was subsequently reprinted in the New York Times, the New York Tribune and other newspapers around the world, and within a short time Koch had gained fame in discovering the cause of a scourge that had affected humankind since recorded history.[7]
In 1890 he obtained a concentrated filtrate of liquid cultures of tubercle bacilli which he called tuberculinand which he believed was to be an effective vaccine for tuberculosis, however after some years of trying, Koch found this not to be so. In 1907 a Viennese paediatrician, Clemens Freiherr von Pirquet, used cutaneous scratch tests of tuberculin, the Pirquet test, to diagnose children with ‘latent tuberculosis’, a term which he introduced. Charles Mantoux, a French physician, in 1908 used tuberculin intradermally, the Mantoux test, which replaced Pirquet’s test. In the 1930’s Florence B. Seibert and Esmond R. Long, two American biochemists, developed a tuberculin purified protein derivative, PPD, which did not produce as many false negative results as ‘Koch’s substance’. Koch was awarded the Nobel Prize in 1905 for his work on tuberculosis. He died in 1910 in Baden-Baden from heart disease.[2,6,7]
Koch initially called his bacillus Tuberclebacillus and after the publication of his 1882 lecture, it became popularly known as Koch’s bacillus and tuberculosis became known as Koch’s disease.[7] The bacillus was officially renamed Bacterium tuberculosis by Friedrich Wilhelm Zopf in 1883, changed to Bacillustuberculosisby Edward Emmanuel Klein in 1884, and to Mycobacterium tuberculosis by K.B. Lehman and R. Neumann in 1896 after considering it to belong to a new genus, Mycobacterium.[12]
Staining of the Bacillus and Acid-Alcohol Fast Bacilli
Mycobacterium tuberculosis, as with other Mycobacteria, has a cell wall consisting of glycolipids and lipids which makes the bacteria resistant to chemicals and enzymes, a property which made staining of the bacterium difficult. Koch initially used methylene-blue in an alkaline solution and Bismark brown as a counterstain. In a paper following his address to the Berlin Physiological Society in 1882 Koch remarked : “Under the microscope the structures of the animal tissues, such as the nucleus and its breakdown products bacillus a brighter red. This was known as the Ziehl- Neelson (ZN) stain. The lipid bacterium cell wall of the bacillus has the property of resisting decolourisation by acid and alcohol and so was known as the acid- alcohol-fast bacillus, AAFB, or acid-fast bacillus, AFB.[7,10]
The Tuberculosis Sanatorium

Fresh air, nutritious food and exercise had been proscribed for phthisis throughout history including by Hippocrates and Aretaeus of Cappadocia. Around the middle of the 19th century, Hermann Brehmer, a German physician, proposed sanatorium treatment (called ‘phthisiotherapy’), an ‘immune’ place where a person could be cured with the aid of fresh rarefied alpine air, plentiful nutritious food, mountain walks, and mountain water douches. Brehmer found such a place in 1857 in a valley in the Sudeten Mountains in Silesia and founded his sanatorium, Heilanstalt (“healing place”), in the village of Göbersdorf. Brehmer’s treatment included walks on mountain trails to a waterfall where the patient stood underneath a cold mountain stream, the ‘forest douche’ or Walddusche, which he supervised personally to counter any objections to the icy water that his patients might give. In the sanatorium his patients were given nutritious food and milk, Hungarian wine with dinner, and French cognac at bedtime. Brehmer published his treatment in 1857 in his work Die Chronische Lungenschwindsucht undTuberkulose der Lunge: Ihre Ursache und ihr Heilung,“The Laws and Healing of Chronic Tuberculosis of theLung”.[2, 6, 14, 15]
Towards the end of the 19th century sanatoria were also built for the poorer classes. They were much less salubrious with plainer food, and the patients had to work and do their own housekeeping. For those who still could not afford a sanatorium, improvisations were made in their home with the patient sleeping outside or in a small outdoor bungalow rugged up against the weather. Rooms in sanatoria were sometimes ventilated with stringent airs – creosote, turpentine and eucalyptus.4 Tuberculosis sanatoria became an important treatment in many countries well into the 20th century and many urban hospitals had open air wards as sanatoria. Sanatoria treatment was often beneficial for patients with minimal disease, but many with severe infection still died.[2, 6]
Other treatments were still being sought, and Paul Ehrlich’s discovery in 1909 that syphilis could be cured with an arsphenamine spurred others on to find a chemotherapeutic agent for tuberculosis. Edward Trudeau, medical superintendant of a sanatorium at Adirondack Cottage on Saranac Lake, New York, and who died of tuberculosis in 1916, stated in a letter posthumously published in the British Journal of Tuberculosis:
My faith in the possibilities of chemotherapy for tuberculosis is based simply on what Ehrlich has demonstrated as possible in syphilis – namely, that a chemical compound could be discovered which killed the germ without injuring the cell … I see no reason why what has been accomplished in the treatment of syphilis should not be attained in tuberculosis.[16]
Pneumothorax and Other Surgical Treatments
From the late 1880’s, sanatoria treatment was supplemented by surgical treatment and collapse therapy, or pneumothorax therapy. The benefit of lung collapse was first suggested in 1771 by Edmond Claude Bourru, librarian, Faculté de Médicine in Paris. In 1885 Edouard Bernard de Cérenville, a Swiss surgeon, and in 1890 Max Schede, a German surgeon, performed thoracoplasty, unilateral partial rib resection to reduce thoracic cavity volume and collapse tuberculous cavities, the principle being to allow them to heal and prevent spread of infection. In 1888 Carlo Forlanini, an Italian physician of Pavia, Lombardy, created the first artificial pneumothorax by collapsing the lung and filling the pleural cavity with nitrogen. Other forms of surgical treatment were used such as lobectomy and segmentectomy, but were commonly complicated by the spread of the infection, fistulas and empyema. In the 1940’s the space created by surgical pneumothorax was filled with oil (‘oleothorax’). After the introduction of streptomycin in 1945 and other anti-tuberculous drugs, all forms of surgical treatment were abandoned in favour of drug treatment.[2,6]
The Development of the X-Ray (the Röntgenogram)

An important contribution to the diagnosis and control of tuberculosis was the discovery in 1895 of X-rays by Wilhelm Konrad von Röntgen. While experimenting with a Crooke’s cathode ray tube Röntgen produced a radiation that could produce shadows of metal objects on a photographic plate. Röntgen’s technique of utilising these rays to show the body’s skeleton with images he called Röntgenograms (he initially called them X-rays but was convinced by his colleagues to change the name) was able to be applied to looking in more detail at internal organs and was very effective at showing tuberculosis in the lung in its various stages, especially the Ghon focus and the apical cavitation and calcification. X-ray screening was introduced for military recruits during World War I and then for the general population through to World War II where it was again used to screen military recruits. Its efficacy in population screening was found to be very low and was ceased in the 1950’s, however it still remained a cheap means of individual diagnostic screening and together with the tuberculin skin sensitivity test played a very significant role in controlling the disease. Röntgen was awarded the Nobel Prize in 1901 for his work.
The Bacille Calmette-Guérin (BCG) Vaccine
In 1900 two French bacteriologists and Pastoriens, Albert Calmette and Camille Guérin, began their research for an antituberculosis vaccine at the Pasteur Institute in Lille. By 1908, by successive sub- culturing a virulent strain of Mycobacterium bovis(previously supplied to them by Edmond Nocard, a French veterinarian and microbiologist) on a medium containing ox bile, they were able to produce a non- virulent strain which they formulated into a live attenuated vaccine. By 1919 Calmette and Guérin showed the effectiveness of their vaccine in animals and called their vaccine Bacille Bilie Calmette- Guérin, later abbreviated to Bacille Calmette-Guérin or BCG. In 1921 the first human administration of BCG was performed by two French physicians, Benjamin Weille-Hallé and Raymond Turpin, at the Charité Hospital, Paris, using an oral vaccine. The vaccine was given to an infant born of a mother who died from tuberculosis shortly after giving birth, the child survived and did not contract the disease. The vaccine soon became popular throughout Europe and over the next seven years over one hundred thousand children were immunised.[2,4,6,17]
In 1930 popular confidence in the vaccine was greatly affected when in Lübeck in Germany 250 children were given a BCG vaccine that had been accidently contaminated by virulent tubercle bacilli, 73 of the children died in the first year from tuberculosis infection and a further 135 were infected but recovered.[6,17] World War II was followed by a resurgence of tuberculosis throughout Europe and Asia and in 1948 UNICEF undertook a tuberculosis control program of tuberculin testing and BCG vaccination in children and many countries followed suit.2 Routine vaccination was discontinued in the 1970’s but is still used in many countries with a high prevalence of tuberculosis to prevent childhood tuberculous meningitis and miliary disease, and for health care and military personnel and other people at high risk of exposure to tuberculosis.[18]
The Development of Streptomycin and Other Anti-Tuberculous Drugs

Tuberculosis was resistant to the sulphonamides of the 1930’s and to penicillin of the 1940’s. In 1940 Selman Waksman, a Ukrainian born American microbiologist working at Rutgers University with funding from chemical company Mercke & Co., isolated actinomycin from actinomycetes fungi and in 1942 streptothricin, but these were too toxic to use. In 1943 Waksman and his colleagues Albert Schatz and Elizabeth Bugie obtained streptomycin from Streptomycesgriseus which was found to be very effective against tuberculosis and much less toxic, and became a standard treatment by 1945. Waksman was awarded the Nobel Prize in 1952 for the discovery. Waksman also coined the term “antibiotic” in 1941 after his discovery of actinomycin.[2,4,6,8,10]
In 1943 Jorgen Lehmann, a Swedish physician, developed para-aminosalicylic acid (PAS) and in 1945 Gerhard Domagk, a German bacteriologist, developed thiosemicarbazone, both also very effective. Since then other anti-tuberculosis antibiotics have been developed such as isoniazid, rifampicin, ethambutol, and pyrazinamide, and more recently, viomycin and ciprofloxacin which are used in drug resistant infections.[2,6]
Tuberculosis and AIDS
In the 1980’s and 1990’s the incidence of tuberculosis surged as a major opportunistic infection in people with HIV infection and AIDS related to their immune system impairment. WHO estimates that in 2012 there were 8.6 million new cases of tuberculosis, of which 1.1 million had HIV co-infection, and 1.3 million died from tuberculosis. The largest number of new cases of tuberculosis occurred in Asia, accounting for 60% of new cases. Sub-Saharan Africa had the highest rate per population with over 260 new cases per 100,000.[19, 20, 21]
The risk of developing tuberculosis is estimated to be between 12-20 times greater in people living with HIV than those without HIV infection. Worldwide 15% of patients with tuberculosis have HIV co-infection, and up to 50-80% have HIV co-infection in parts of sub- Saharan Africa. Tuberculosis is the leading cause of death in people with HIV infection and AIDS, 1 in 3 people with AIDS die from tuberculosis.[21, 22] The incidence of HIV-related tuberculosis has declined in developed countries due to effective anti-TB and anti-HIV treatment, but remains a significant health problem in many developing countries.
Drug-Resistant Tuberculosis
In recent decades multidrug resistant tuberculosis (MDR-TB), tuberculosis which does not respond to at least isoniazid and rifampicin, has emerged and is present in most countries. In 2012 WHO estimated there to be 450,000 cases worldwide, most of which were in India, China and the Russian Federation, and 10% had extensively drug resistant tuberculosis (XDR-TB). MDR-TB is on the rise in many countries, but an international initiative financed by UNITAID is currently making progress in improving access in participating countries to diagnostic services for tuberculosis and HIV, and especially to diagnosis of MDR-TB.[19, 20, 23, 24]
Tuberculosis and the Military

Tuberculosis was a major problem in soldiers of the Crimean War of 1853-1856. Florence Nightingale in her paper On Army Sanitary Reform under the LateLordHerbert read at the CongrésInternational deBienfaisance on 13 June 1862 remarked :
After the Crimean War, it was found that the death rate among soldiers from consumption alone and its cognate diseases (the monstrous product of breathing foul air) exceeded the death rate from all causes among the civil population.[25]
Tuberculosis as a medicomilitary problem became more apparent during World War I. Both the Allies and the Germans screened their military recruits for tuberculosis using chest radiographs, however many were still enlisted with latent or active tuberculosis. Before the war ended, 2,000 soldiers had died of tuberculosis in the US Army and was the leading cause of discharge.[2, 25] After World War I the US Army established the Fitzsimons Army Hospital in Denver, Colorado, to cope with the large number of returning Army and Navy veterans with tuberculosis.
Tuberculosis declined in incidence between the two world wars due to better case finding, early diagnosis, and better conditions of living, although X-ray screening was used again during World War
II. During the years 1942 to 1945 there were 3,099 soldiers discharged from the US Army for tuberculosis, just over half of all discharges. In one half of those discharges the disease had already been present on enlistment. [26] In 1943 the Valley Forge Hospital was established in Phoenixville, Pennsylvania, to treat returning US military personnel including those with tuberculosis. Following the introduction of streptomycin and other anti-tuberculous drugs, the worldwide prevalence of tuberculosis declined and remained low until its resurgence with HIV in the 1980’s.
In the last several decades microepidemics have occurred in small close knit units on US and British Naval ships and land based units deployed overseas. In 1998 an outbreak of 21 cases of active tuberculosis occurred among the ship’s sailors and the marine expeditionary unit on a US amphibious ship.27 In 2006 a small outbreak occurred on HMS Ocean, several naval personnel had active tuberculosis and 80 cases of latent infection were identified.28 In 2006 a sailor on USS Ronald Reagan was diagnosed with active pulmonary tuberculosis and 139 sailors and 1 civilian were identified with new latent tuberculosis.[29]
Overall incidence of tuberculosis in Western militaries is currently low but is higher in militaries of other countries such as South Korea and the Russian Federation. Mancuso & Aaron28 in an analysis of US active military personnel from 1998 to 2012 found that the average annual incidence rate of pulmonary tuberculosis was only 0.6 per 100,000, which was one fifth of the incidence in the US general population. The rate declined from 1.5 per 100,000 in 1998 to 0.35 per 100,000 in 2012. In health care personnel in 2012 the rate was 0.46 per 100,000, an increased risk of 28%, however this was not statistically significant. Interestingly, and reminiscent of the early 20th century experiences, the most common factor associated with diagnosis during military service was latent infection at the time of enlistment. Military personnel are still at significant risk of acquiring tuberculosis infection because of living and working in close quarters and deployment in regions with a high prevalence of tuberculosis such as Afghanistan, Iraq and South- East Asia, and are particularly at risk of exposure to multidrug resistant tuberculosis (MDR-TB).[27, 30, 31]
Tuberculosis has been a severe health problem throughout recorded human history, and probably for many thousands of years before that. It has been known by many names including phthisis, consumption, the “white plague” and “the robber of youth”. The disease had been romanticised in the 19th century by people such as John Keats, Edgar Allen Poe and Emily Brontë. The nature, cause and cure of the disease had eluded the scientific and medical community until the discoveries by eminent scientists such as René Laennec, Jean Antoine Villemin, Robert Koch and Selman Waksman. Tuberculosis never-the-less remains a significant public health problem worldwide, especially with the emergence of multidrug resistant tuberculosis, and also remains an important medicomilitary issue.
Notes
Phthisis, Consumption, and the White Plague
- Herzog H. History of tuberculosis. Respiration 1998; 65: 5-15. Available at : https://www.karger.com/ Article/PDF/29220, accessed on 11.9.10.
- Daniel TM. The history of tuberculosis. Resp Med 2006; 100: 1862-1870. Available at : https://www. resmedjournal.com/article/S0954-6111(06)00401-X/fulltext, accessed on 11.9.13.
- Boire NA, Riedel VAA, Parrish NM, et al. Tuberculosis: from an untreatable disease in antiquity to an untreatable disease in modern times. J Anc Dis Prev Rem 2013; 1 (2): 1-11. Available at : https://www. esciencecentral.org/journals/2329-8731/2329-8731-1-106.pdf , accessed on 11.9.13.
- Dormandy T. The White Death: A History of Tuberculosis. London: The Hambledon Press, 1999, p. xiv, 2, 4, 13, 34-36, 73-84, 92-94, 101-104, 129-137, 147, 392.
- Dubos R, Dubos J. The White Plague: Tuberculosis, Man and Society. Boston; Little, Brown & Co., 1952, p. 7, 10, 13-14, 70-73, 91, 98, 203.
- Segen JC. The Dictionary of Modern Medicine. Park Ridge, NJ; Parthenon, 1992, p. 783.
- Bunyan J. The Life and Death of Mr. Badman. Acacia John Bunyan Online Library. 2013. Available at : https://acacia.pair.com/Acacia.John.Bunyan/Sermons.Allegories/Life.Death.Badman/XVIII.html , accessed on 18.10.13
- National Institute of Health (U.S.) Tuberculosis (TB). 2010. Available at : https://www.niaid.nih.gov/ topics/tuberculosis/Understanding/history/pages/historical/ , accessed on 18.10.13.
- Bynum H. Spitting Blood. Oxford; Oxford University Press, 2012, p. 13, 17, 18, 33-39, 56-62, 104, 106- 107, 110.
- Long ER. Tuberculosis in World War I. In : Hays SB (Editor-in-chief). Preventive Medicine in World War II. Vol IV. Communicable Diseases. Washington, DC; Office of the Surgeon General, Department of the Army, 1958. Available at : https://history.amedd.army.mil/booksdocs/wwii/PM4/CH14.Tuberculosis. htm, accessed on 13.9.13.
- Mancuso JD. Tuberculosis trends in the U.S. Armed Forces, active component. Medical Surveillance Monthly Report 2013; 20 (5): 4-8. Available at : https://www.afhsc.mil/viewMSMR?file=2013/v20_n05. pdf, accessed on 13.9.13.
- O’Shea MK, Wilson D. Tuberculosis and the military. J R Army Med Corps 2013; 159 (3): 190-199. Available at : https://jramc.bmj.com/content/159/3/190.full, accessed on 2.10.13.
- Schreiber W, Mathys FK. Infectio. Basle, Switzerland: Editione Roche, 1987, p. 181-193.
- Hippocrates (460-370 BCE). Book 1 – Of the Epidemics. In : Adams F (translator). The Genuine Works of Hippocrates. London: The Sydenham Society, 1849. [Facsimile edition, The Classics of Medicine Library, Alabama, 1985, p. 352-354.]
- Daniel TM. Pioneers in Medicine and their Impact on Tuberculosis. Rochester, NY; University of Rochester Press, 2000, p. 4, 29, 46-48, 50-51, 74-76.
- Pease AS. Some remarks on the diagnosis and treatment of tuberculosis in antiquity. Isis 1940; 31 (2): 380-393. Available at : https://www.jstor.org/discover/10.2307/225758?uid=3737536&uid=2&uid=4&s id=21102645880757, accessed on 11.9.13
- Garrison FH. An Introduction to the History of Medicine. Philadelphia & London: W B Saunders & Co., 1921, p. 109, 288, 411-413, 616.
- Major RH. Classic Descriptions of Disease. Springfield, USA: Charles C Thomas, 1932, p. 49-56, 56-57, 58-61, 61-62.
- Roguin A. René Théophile Hyacinthe Laënnec (1781-1826): the man behind the stethoscope. Clin Med Res 2006; 4 (3): 230-235. Available at : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1570491/ pdf/0040230.pdf, accessed on 11.9.13.
- Nuland SB. Doctors: The Illustrated History of Medical Pioneers. New York: Black Dog & Leventhal Publishers, 1988, p. 193-227.
- Nixon JA. Classification of adventitious sounds. [Letter] BMJ 16 April 1938, p. 170. Available at : https:// europepmc.org/articles/PMC2086242/pdf/brmedj04272-0043a.pdf , accessed on 19.10.13.
- Barlow F. The King’s Evil. English Historical Reviews (1980). XCV (CCCLXXIV): 3-27. Available at : https://ehr.oxfordjournals.org/content/XCV/CCCLXXIV/3.full.pdf+html, accessed on 17.9.13.
- Goddard PR. The King’s Evil. West of England Medical Journal 2013; 112 (2): Article 3 (e-journal). Available at : file:///C:/Documents%20and%20Settings/Owner/My%20Documents/Downloads/3)_The_ Kings_Evil_The_Royal_Touch_for_Scrofula.pdf , accessed on 20.5.14.
- Robert Koch and Tuberculosis. NobelPrize.org. 21 September 2003. Available at : https://www.nobelprize. org/educational/medicine/tuberculosis/readmore.html, accessed on 11.9.13.
- Dobson M. Disease. London: Quercus, 2007.
- Murray JF. The White Plague: down, and out, or up and coming? Am Rev Respir Dis 1989; 140 (6): 1788- 1795. Available at : https://www.atsjournals.org/doi/abs/10.1164/ajrccm/140.6.1788?journalCode=ar rd , accessed on 18.10.13.
- Evans R. The White Plague. 2012. Available at : https://www.gresham.ac.uk/lectures-and-events/the- white-plague , accessed on 11.9.13.
- Byrne K. Tuberculosis and the Victorian Literary Imagination. Cambridge; Cambridge University Press, 2011, p. 21, 94, 126.
- Daniel TM. Hermann Brehmer and the origins of tuberculosis sanatoria. In J Tuberc Lung Dis 2011; 15 (2): 161-162. Available at : https://docstore.ingenta.com/cgi-bin/ds_deliver/1/u/d/ISIS/75571322.1/ iuatld/ijtld/2011/00000015/00000002/art00004/6E464163097468501379918384891BF294582C38 3B.pdf?link=https://www.ingentaconnect.com/error/delivery&format=pdf , accessed on 11.9.13.
- Daniel TM. Pioneers in Medicine and Their Impact on Tuberculosis. Suffolk, UK; University of Rochester Press, 2000, p. 7-8.
- Knopf SA. Hermann Brehmer, and the Semi-centennial Celebration of Brehmer’s Sanitorium for the Treatment of Consumptives; the first Institution of its Kind. New York Medical Journal and Philadelphia Medical Journal, 2 July 1904. Charlestown, SC; Bibliolife Reproduction.
- Sakula A. Robert Koch: centenary of the discovery of the tubercle bacillus, 1882. Thorax 1982; 37: 246-251. Available at : https://thorax.bmj.com/content/37/4/246.full.pdf , accessed on 11.9.1
The Sanatoria and the Discoveries of the Tubercle Bacillus
- Robert Koch and Tuberculosis. NobelPrize.org. 21 September 2003. Available at : https://www.nobelprize. org/educational/medicine/tuberculosis/readmore.html, accessed on 11.9.13.
- Daniel TM. The history of tuberculosis. Resp Med 2006; 100: 1862-1870. Available at : https://www. resmedjournal.com/article/S0954-6111(06)00401-X/fulltext, accessed on 11.9.13.
- Segen JC. The Dictionary of Modern Medicine. Park Ridge, NJ; Parthenon, 1992, p. 783.
- Bynum H. Spitting Blood. Oxford: Oxford University Press, 2012, p. 109-115, 128-145, 166, 175-187, 190-196.
- Dormandy T. The White Death: A History of Tuberculosis. London: The Hambledon press, 1999, p. 54-57, 73-84.
- Herzog H. History of tuberculosis. Respiration 1998; 65: 5-15. Available at : https://www.karger.com/ Article/PDF/29220, accessed on 11.9.10.
- Sakula A. Robert Koch: centenary of the discovery of the tubercle bacillus, 1882. Thorax 1982; 37: 246-251. Available at : https://thorax.bmj.com/content/37/4/246.full.pdf , accessed on 11.9.13.
- Daniel TM. Pioneers in Medicine and their Impact on Tuberculosis. Rochester, NY; University of Rochester Press, 2000, p. 74-76, 179.
- Garrison F H. An Introduction to the History of Medicine. Philadelphia & London: W B Saunders & Co., 1921, p. 578-590, 721.
- Boire NA, Riedel VAA, Parrish NM, et al. Tuberculosis: from an untreatable disease in antiquity to an untreatable disease in modern times. J Anc Dis Prev Rem 2013; 1 (2): 1-11. Available at : https://www. esciencecentral.org/journals/2329-8731/2329-8731-1-106.pdf , accessed on 11.9.13.
- Brock TD. Robert Koch. A life in medicine and bacteriology. New York: Springer-Verlag, 1988, page 129.
- UniProt Taxonomy. Mycobacterium tuberculosis. 2013. Available at : https://www.uniprot.org/ taxonomy/1773, accessed on 11.9.13.
- National Institute of Health (U.S.) Tuberculosis (TB). 2010. Available at : https://www.niaid.nih.gov/ topics/tuberculosis/Understanding/history/pages/historical/ , accessed on 18.10.13.
- Daniel TM. Hermann Brehmer and the origins of tuberculosis sanatoria. Int J Tuberc Lung Dis 2011; 15 (2): 161-162. Available at : https://docstore.ingenta.com/cgi-bin/ds_deliver/1/u/d/ISIS/75571322.1/ iuatld/ijtld/2011/00000015/00000002/art00004/6E464163097468501379918384891BF294582C38 3B.pdf?link=https://www.ingentaconnect.com/error/delivery&format=pdf , accessed on 11.9.13.
- Kinghorn HM. Hermann Brehmer. Trans Am Climatol Clin Assoc 1921; 37: 193-210. Available at : https:// europepmc.org/articles/PMC2307432/pdf/tacca200003-0222.pdf , accessed on 11.9.13.
- Trudeau EL. Relative immunity in tuberculosis and the use of tuberculin. Br J Tuberc 1916; 10: 29-30. Available at : https://ac.els-cdn.com/S0366085016800149/1-s2.0-S0366085016800149-main.pdf?_ tid=d4ea0b70-23e9-11e3-bd63-00000aab0f01&acdnat=1379897476_57f5328534c5819d162afb08d9b14 d0b , accessed on 23.9.13.
- Luca S, Mihaescu, T. History of BCG vaccine. Maedica (Buchar.) 2013; 8 (1): 53-58. Available at : https:// www.ncbi.nih.gov/pmc/articles/PMC3749764 , accessed on 1.5.14.
- Centers for Disease Control and Prevention. BCG Vaccine. 2011. Available at : https://www.cdc.gov/tb/ publications/factsheets/prevention/bcg.htm , accessed on 1.5.14.
- World Health Organisation. WHO Global Tuberculosis Report 2012. Available at : https://www.who.int/ tb/publications/factsheet_global.pdf , accessed on 26.9.13.
- World Health Organisation. Tuberculosis. Fact sheet No. 104. 2014. Available at : https://www.who.int/ mediacentre/factsheets/fs104/en/ , accessed on 1.5.14.
- World Health Organisation. Tuberculosis and HIV. 2014. Available at : https://www.who.int/hiv/topics/ tb/en/ accessed on 1.5.14.
- Leutkemeyer A. Tuberculosis and HIV. University of California, San Francisco. Available at : https://www. hivinsite.ucsf.edu/InSite?page=kb-05-01-06#S3X , accessed on 1.5.14.
- World Health Organisation. Progress in diagnosing multidrug-resistant tuberculosis. 2014. Available at https://www.who.int/medicacentre/news/releases/2014/tb-day/en/ , accessed on 1.5.14.
- Matteelli A, Centis R, D’Ambrosio L, et al. Multidrug-resistant tuberculosis today. Bulletin of the World Health Organisation 2012; 90: 78, available at https://www.who.int/bulletin/volumes/90/2/11-097360/ en/, accessed on 1.5.14.
- Warren P. The Evolution of the Sanatorium: the First Half-Century, 1854-1904. Can Bull Med Hist 2006; 23 (2): 457-470. Available at : https://www.cbmh.ca/index.php/cbmh/article/viewFile/1239/1230 , accessed on 11.9.13.
- Long ER. Tuberculosis in World War I. In : Hays SB (Editor-in-chief). Preventive Medicine in World War II. Vol IV. Communicable Diseases. Washington, DC; Office of the Surgeon General, Department of the Army, 1958. Available at : https://history.amedd.army.mil/booksdocs/wwii/PM4/CH14.Tuberculosis. htm, accessed on 13.9.13.
- LaMar JE, Malakooti MA. Tuberculosis outbreak investigation of a U.S. Navy amphibious ship crew and Marine expeditionary unit aboard, 1998. [Abstract] Mil Med 2003; 168 (7): 523-527. Available at : https:// www.ncbi.nlm.nih.gov/pubmed/12901459 , accessed on 2.10.13.
- O’Shea MK, Wilson D. Tuberculosis and the military. J R Army Med Corps 2013; 159 (3): 190-199. Available at : https://jramc.bmj.com/content/159/3/190.full, accessed on 2.10.13.
- Buff AM, Deshpande SJ, Harrington TA, et al. Investigation of Mycobacterium tuberculosis infection transmission aboard the U.S.S. Ronald Reagan, 2006. Mil Med 2008; 173 (6): 588-593. Available at : https://www.redorbit.com/news/health/1478948/investigation_of_mycobacterium_tuberculosis_ transmission_aboard_the_uss_ronald_reagan/ , accessed on 2.10.2013.
- Mancuso JD, Aaron CL. Tuberculosis trends in the U.S. Armed Forces, active component. Medical Surveillance Monthly Report 2013; 20 (5): 4-8. Available at : https://www.afhsc.mil/viewMSMR?file=2013/ v20_n05.pdf , accessed on 13.9.13.
- Freier G, Wright A, Nelson G, et al. Multidrug-resistant tuberculosis in military recruits. Emerg Inf Dis 2006; 12 (5): 760-762. Available at : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3374445/pdf/05- 0708.pdf , accessed on 13.9.13
Originally published by the Journal of Military and Veterans’ Health (22:2, June 2014 and 22:2, June 2014) under the terms of a Creative Commons Attribution 4.0 International license.