

By John Frith
The Three Great Pandemics
Overview
Plague is an acute infectious disease caused by the bacillus Yersinia pestis and is still endemic in indigenous rodent populations of South and North America, Africa and Central Asia. In epidemics plague is transmitted to humans by the bite of the Oriental or Indian rat flea and the human flea. The primary hosts of the fleas are the black urban rat and the brown sewer rat. Plague is also transmissible person to person when in its pneumonic form. Yersinia pestis is a very pathogenic organism to both humans and animals and before antibiotics had a very high mortality rate. Bubonic plague also has military significance and is listed by the Centers for Disease Control and Prevention as a Category A bioterrorism agent.[1]
There have been three great world pandemics of plague recorded, in 541, 1347, and 1894 CE, each time causing devastating mortality of people and animals across nations and continents. On more than one occasion plague irrevocably changed the social and economic fabric of society.
In most human plague epidemics, infection initially took the form of large purulent abscesses of lymph nodes, the bubo (L. bubo = ‘groin’, Gr. boubon = ‘swelling in the groin’), this was bubonic plague. When bacteraemia followed, it caused haemorrhaging and necrosis of the skin rapidly followed by septicaemic shock and death, septicaemic plague. If the disease spread to the lung through the blood, it caused an invariably fatal pneumonia, pneumonic plague, and in that form plague was directly transmissible from person to person.
The three great plague pandemics had different geographic origins and paths of spread. The Justinian Plague of 541 started in central Africa and spread to Egypt and the Mediterranean. The Black Death of 1347 originated in Asia and spread to the Crimea then Europe and Russia. The third pandemic, that of 1894, originated in Yunnan, China, and spread to Hong Kong and India, then to the rest of the world.[2]
The causative organism, Yersinia pestis, was not discovered until the 1894 pandemic and was discovered in Hong Kong by a French Pastorien bacteriologist, Alexandre Yersin. Four years later in 1898 his successor, Paul-Louis Simond, a fellow Asia and migrated westward on the sea routes from China and India. The brown rat flourished in Europe where there were open sewers and ample breeding grounds and food and in the 18th and 19th centuries replaced the black rat as the main disease host.[4][9]
The primary vectors for transmission of the disease from rats to humans were the Oriental or Indian rat flea, Xenopsylla cheopis, and the Northern or European rat flea, Nosopsyllus fasciatus. The human flea, Pulex irritans, and the dog and cat fleas, Ctenocephalides canis and felis, were secondary vectors. In the pandemics, the infected fleas were able to spread the plague over long distances as they were carried by rats and by humans travelling along trade routes at sea and overland, and also by infesting rice and wheat grain, clothing, and trade merchandise. When infected, the proventriculus of the flea becomes blocked by a mass of bacteria. The flea continues to feed, biting with increasing frequency and agitation, and in an attempt to relieve the obstruction the flea regurgitates the accumulated blood together with a mass of Yersinia pestis bacilli directly into the bloodstream of the host. The fleas multiply prolifically on their host and when the host dies they leave immediately, infesting new hosts and thus creating the foundations for an epidemic.[10][11]
The Justinian Plague of 541-544

The first great pandemic of bubonic plague where people were recorded as suffering from the characteristic buboes and septicaemia was the Justinian Plague of 541 CE, named after Justinian I, the Roman emperor of the Byzantine Empire at the time. The epidemic originated in Ethiopia in Africa and spread to Pelusium in Egypt in 540. It then spread west to Alexandria and east to Gaza, Jerusalem and Antioch, then was carried on ships on the sea trading routes to both sides of the Mediterranean, arriving in Constantinople (now Istanbul) in the autumn of 541.[12][13]
The Byzantine court historian, Procopius of Caesarea, in his work History of the Wars, described people with fever, delirium and buboes He wrote that the epidemic was one ‘by which the whole human race came near to be annihilated’. Procopius wrote of the symptoms of the disease :
“ … with the majority it came about that they were seized by the disease without becoming aware of what was coming either through a waking vision or a dream. … They had a sudden fever, some when just roused from sleep, others while walking about, and others while otherwise engaged, without any regard to what they were doing. And the body showed no change from its previous colour, nor was it hot as might be expected when attacked by a fever, nor indeed did any inflammation set in, but the fever was of such a languid sort from its commencement and up till evening that neither to the sick themselves nor to a physician who touched them would it afford any suspicion of danger. It was natural, therefore, that not one of those who had contracted the disease expected to die from it. But on the same day in some cases, in others on the following day, and in the rest not many days later, a bubonic swelling developed; and this took place not only in the particular part of the body which is called boubon, that is, “below the abdomen,” but also inside the armpit, and in some cases also beside the ears, and at different points on the thighs.”[14]
The focus of the Justinian pandemic was Constantinople, reaching a peak in the spring of 542 with 5,000 deaths per day in the city, although some estimates vary to 10,000 per day, and it went on to kill over a third of the city’s population. Victims were too numerous to be buried and were stacked high in the city’s churches and city wall towers, their Christian doctrine preventing their disposal by cremation. Over the next three years plague raged through Italy, southern France, the Rhine valley and Iberia. The disease spread as far north as Denmark and west to Ireland, then further to Africa, the Middle East and Asia Minor. Between the years 542 and 546 epidemics in Asia, Africa and Europe killed nearly 100 million people.[15][16]
The pandemic had a drastic effect and permanently changed the social fabric of the Western world. It contributed to the demise of Justinian’s reign. Food production was severely disrupted and an eight year famine followed. The agrarian system of the empire was restructured to eventually become the three field feudal system. The social and economic disruption caused by the pandemic marked the end of Roman rule and led to the birth of culturally distinctive societal groups that later formed the nations of medieval Europe.[12]
Further major outbreaks occurred throughout Europe and the Middle East over the next 200 years – in Constantinople in the years 573, 600, 698 and 747, in Iraq, Egypt and Syria in the years 669, 683, 698, 713, 732 and 750 and Mesopotamia in 686 and 704. In 664 plague laid waste to Ireland, and in England it came to be known as the Plague of Cadwaladyr’s Time, after a Welsh king who contracted plague but survived it in 682. The plague continued in intermittent cycles in Europe into the mid-8th century and did not re-emerge as a major epidemic until the 14th century.
The ‘Black Death’ of Europe in 1347 to 1352

The Black Death of 1347 was the first major European outbreak of the second great plague pandemic that occurred over the 14th to 18th centuries. In 1346 it was known in the European seaports that a plague epidemic was present in the East. In 1347 the plague was brought to the Crimea from Asia Minor by the Tartar armies of Khan Janibeg, who had laid siege to the town of Kaffa (now Feodosya in Ukraine), a Genoese trading town on the shores of the Black Sea. The siege of the Tartars was unsuccessful and before they left, from a description by Gabriel de Mussis from Piacenza, in revenge they catapulted over the walls of Kaffa corpses of people who had died from the Black Death. In panic the Genoese traders fled in galleys with ‘sickness clinging to their bones’ to Constantinople and across the Mediterranean to Messina, Sicily, where the great pandemic of Europe started. By 1348 it had reached Marseille, Paris and Germany, then Spain, England and Norway in 1349, and eastern Europe in 1350. The Tartars left Kaffa and carried the plague away with them spreading it further to Russia and India.[17]
A description of symptoms of the plague was given by Giovanni Boccaccio in 1348 in his book Decameron, a set of tales of a group of Florentines who secluded themselves in the country to escape the plague :
“.. in men and women alike it first betrayed itself by the emergence of certain tumours in the groin or armpits. Some of which grew as large as a common apple, others as an egg, some more, some less, which the common folk called gavocciolo. From the two said parts of the body this deadly gavocciolo soon began to propagate and spread itself in all directions indifferently; after which the form of the malady began to change, black spots or livid making their appearance in many cases on the arm or the thigh or elsewhere,..“[17]
The term “Black Death” was not used until much later in history and in 1347 was simply known as “the pestilence” or “pestilentia”, and there are various explanations of the origin of the term. Butler [11] states the term refers to the haemorrhagic purpura and ischaemic gangrene of the limbs that sometimes ensued from the septicaemia. Ziegler17 states it derives from the translation of the Latin pestis atra or atra mors, ‘atra’ meaning ‘terrible’ or ‘dreadful’, the connotation of which was ‘black’, and ‘mors’ meaning ‘death’, and so ‘atra mors’ was translated as meaning ‘black death’.
The social impacts of the Black Death in Europe during the 14th century
The overall mortality rate varied from city to city, but in places such as Florence as observed by Boccaccio up to half the population died, the Italians calling the epidemic the mortalega grande, ‘the great mortality’.[18] People died with such rapidity that proper burial or cremation could not occur, corpses were thrown into large pits and putrefying bodies lay in their homes and in the streets. People were as much afraid they would suffer a spiritual death as they were a physical death since there were no clergy to perform burial rites:
“Shrift there was none; churches and chapels were open, but neither priest nor penitents entered – all went to the charnelhouse. The sexton and the physician were cast into the same deep and wide grave; the testator and his heirs and executors were hurled from the same cart into the same hole together.”[18]

Transmission of the disease was thought to be by miasmas, disease carrying vapours emanating from corpses and putrescent matter or from the breath of an infected or sick person. Others thought the Black Death was punishment from God for their sins and immoral behaviour, or was due to astrological and natural phenomena such as earthquakes, comets, and conjunctions of the planets. People turned to patron saints such as St Roch and St Sebastian or to the Virgin Mary, or joined processions of flagellants whipping themselves with nail embedded scourges and incanting hymns and prayers as they passed from town to town.[17][19][20]
“When the flagellants – they were also called cross brethren and cross bearers – entered a town, a borough or a village in a procession their entry was accompanied by the pealing of bells, singing, and a huge crowd of people. As they always marched two abreast, the procession of the numerous penitents reached farther than the eye could see.”[20]
The only remedies were inhalation of aromatic vapours from flowers and herbs such as rose, theriaca, aloe, thyme and camphor. Soon there was a shortage of doctors which led to a proliferation of quacks selling useless cures and amulets and other adornments that claimed to offer magical protection.
In this second pandemic, plague again caused great social and economic upheaval. Often whole families were wiped out and villages abandoned. Crops could not be harvested, travelling and trade became curtailed, and food and manufactured goods became short. As there was a shortage of labour, surviving villager labourers, the ‘villeins’, extorted exorbitant wages from the remaining aristocratic landowners. The villeins prospered and acquired land and property. The plague broke down the normal divisions between the upper and lower classes and led to the emergence of a new middle class.[9][17] The plague lead to a preoccupation with death as evident from macabre artworks such as the ‘Triumph of Death’ by Pieter Breughel the Elder in 1562, which depicted in a panoramic landscape armies of skeletons killing people of all social orders from peasants to kings and cardinals in a variety of macabre and cruel ways.
In the period 1347 to 1350 the Black Death killed a quarter of the population in Europe, over 25 million people, and another 25 million in Asia and Africa.[15] Mortality was even higher in cities such as Florence, Venice and Paris where more than half succumbed to the plague. A second major epidemic occurred in 1361, the pestis secunda, in which 10 to 20% of Europe’s population died.13 Other virulent infectious disease epidemics with high mortalities occurred during this time such as smallpox, infantile diarrhoea and dysentery. By 1430, Europe’s population was lower than it had been in 1290 and would not recover the pre-pandemic level until the 16th century.[13][21]
Quarantine

In 1374 when another epidemic of the Black Death re-emerged in Europe, Venice instituted various public health controls such as isolating victims from healthy people and preventing ships with disease from landing at port. In 1377 the republic of Ragusa on the Adriatic Sea (now Dubrovnik in Yugoslavia) established a ships’ landing station far from the city and harbour in which travellers suspected to have the plague had to spend thirty days, the trentena, to see whether they became ill and died or whether they remained healthy and could leave. The trentena was found to be too short and in 1403 in Venice, travellers from the Levant in the eastern Mediterranean were isolated in a hospital for forty days, the quarantena or quaranta giorni, from which we derive the term quarantine.8,18 This change to forty days may have also been related to other biblical and historical references such as the Christian observance of Lent, the period for which Christ fasted in the desert, or the ancient Greek doctrine of “critical days” which held that contagious disease will develop within 40 days after exposure.[22] In the 14th and 15th centuries following, most countries in Europe had established quarantine, and in the 18th century Habsburg established a cordon sanitaire, a line between infected and clean parts of the continent which ran from the Danube to the Balkans. It was manned by local peasants with checkpoints and quarantine stations to prevent infected people from crossing from eastern to western Europe.[8]
The leather costume of the plague doctors at Nijmegen
In the 15th and 16th centuries doctors wore a peculiar costume to protect themselves from the plague when they attended infected patients, first illustrated in a drawing by Paulus Furst in 1656 and later Jean-Jacques described a similar costume worn by the plague doctors at Nijmegen, an old Dutch town in Gelderland, in his 1721 work Treatise on the Plague. They wore a protective garb head to foot with leather or oil cloth robes, leggings, gloves and hood, a wide brimmed hat which denoted their medical profession, and a beak like mask with glass eyes and two breathing nostrils which was filled with aromatic herbs and flowers to ward off the miasmas. They avoided contact with patients by taking their pulse with a stick or issued prescriptions for aromatic herb inhalations passing them through the door, and buboes were lanced with knives several feet long.[19]
The Great Plague of London of 1665 to 1666
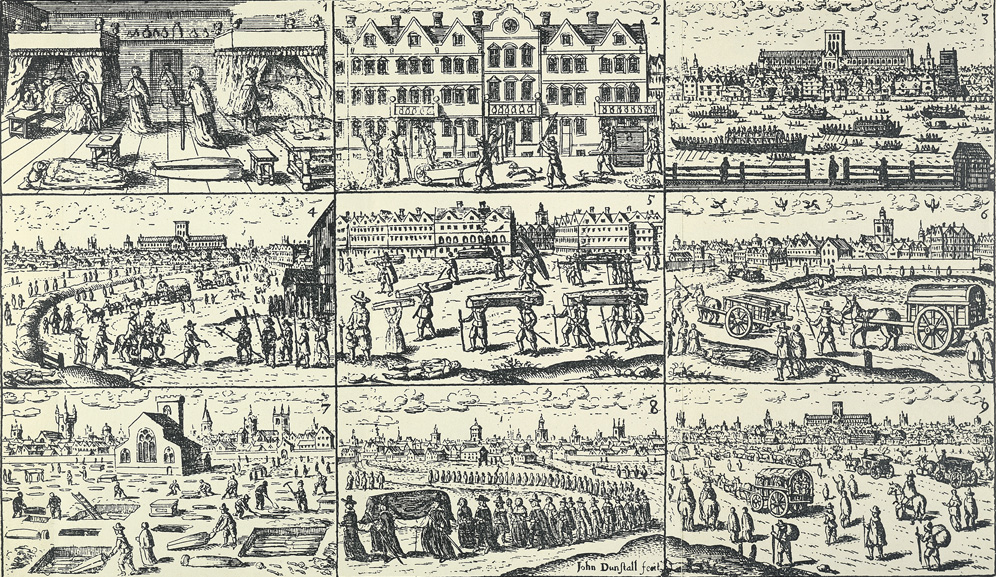
Plague continued to occur in small epidemics throughout the world but a major outbreak of the pneumonic plague occurred in Europe and England in 1665 to 1666. The epidemic was described by Samuel Pepys in his diaries in 1665 and by Daniel Defoe in 1722 in his A Journal of a Plague Year. People were incarcerated in their homes, doors painted with a cross. The epidemic reached a peak in September 1665 when 7,000 people per week were dying in London alone. Between 1665 and 1666 a fifth of London’s population died, some 100,000 people.[17] The Great Fire of London in 1666 and the subsequent rebuilding of timber and thatch houses with brick and tile disturbed the rats’ normal habitat and led to a reduction in their numbers, and may have been a contributing factor to the end of the epidemic.[9]
An old English nursery rhyme published in Kate Greenaway’s book Mother Goose 1881 reminds us of the symptoms of the plague :
‘Ring, a-ring, o’rosies, (a red blistery rash)
A pocket full of posies (fragrant herbs and flowers to ward off the ‘miasmas’)
Atishoo, atishoo (the sneeze and the cough heralding pneumonia)
We all fall down.’ (all dead)
Plague waxed and waned in Europe until the late 18th century, but not with the virulence and mortality of the 14th century European Black Death.
The Third Pandemic of 1894

The plague re-emerged from its wild rodent reservoir in the remote Chinese province of Yunnan in 1855. From there the disease advanced along the tin and opium routes and reached the provincial capital of K’unming in 1866, the Gulf of Tonkin in 1867, and the Kwangtung province port of Pakhoi (now Pei-hai) in 1882. In 1894 it had reached Canton and then spread to Hong Kong. It had spread to Bombay by 1896 and by 1900 had reached ports on every continent, carried by infected rats travelling the international trade routes on the new steamships.[3][23] It was in Hong Kong in 1894 that Alexandre Yersin discovered the bacillus now known as Yersinia pestis, and in Karachi in 1898 that Paul-Louis Simond discovered the brown rat was the primary host and the rat flea the vector of the disease.[3][4][24][25]
In 1900 the plague came to Australia where the first major outbreak occurred in Sydney, its epicentre at the Darling Harbour wharves, spreading to the city, Surry Hills, Glebe, Leichhardt, Redfern, and The Rocks, and causing 100 deaths. John Ashburton- Thompson, the chief medical officer, recorded the epidemic and confirmed that rats were the source and their fleas were the vectors in the epidemic. There were 12 major outbreaks of plague in Australia from 1900 to 1925 with 1371 cases and 535 deaths, most cases occurring in Sydney.[26]
The third pandemic waxed and waned throughout the world for the next five decades and did not end until 1959, in that time plague had caused over 15 million deaths, the majority of which were in India. There have been outbreaks of plague since, such as in China and Tanzania in 1983, Zaire in 1992, and India, Mozambique and Zimbabwe in 199415.[27] In Madagascar in the mid-1990’s, a multi-drug resistant strain of the bacillus was identified15, 28. Currently around 2,000 cases occur annually, mostly in Africa, Asia and South America, with a global case fatality rate of 5% to 15%.[28]
Bubonic plague is a virulent disease with a significant mortality rate, transmitted primarily by the bite of the rat flea or through person-to-person when in its pneumonic form. There have been innumerable epidemics of plague throughout history, but it was the pandemics of the 6th, 14th and 20th centuries that have had the most impact on human society, not only in terms of the great mortalities, but also the social, economic and cultural consequences that resulted. The course of development of communities and nations was altered several times. Much has changed to prevent the recurrence of pandemic plague, such as the development of the germ theory and the science of bacteriology, public health measures such as quarantine, and antibiotics such as streptomycin, but plague today is still an important and potentially serious threat to the health of people and animals.
The Discoveries of the Plague Bacillus and Its Vector

There is a close association between infectious diseases, epidemics and war, and for many reasons. In history, soldiers and sailors have endured many hardships – wounds and death, exhaustion from battles and long marches, shortage of shelter, food and water, and sometimes they brought disease with them from their homeland or from other wars, all leaving them susceptible to the added mortality of contagion.[1][2] By the 18th century, many physicians and military surgeons realised the importance of preventing disease and improving the health of soldiers in winning war campaigns.[3] Plague was particularly important because it was known to be highly contagious and caused severe epidemics that had high mortality, although until the discoveries made during the 1894 pandemic, its cause, means of transmission and prevention were not known. Bubonic plague is now a treatable and immunisable disease but it continues to have military significance, especially because of its virulence and infectivity in the pneumonic form, and is listed by the Centers for Disease Control and Prevention as a Category A bioterrorism agent.[4]
For many centuries infectious diseases such as bubonic plague, smallpox and cholera were thought to be due to ‘miasmas’, disease carrying vapours that emanated from corpses, putrescent matter, or the breath of a sick person. Others thought plagues such as the Black Death were due to earthquakes or comets, or were punishment from God for their sins and immoral behaviour. During times of plague, many people prayed to saints such as St Roch and St Sebastian for salvation or became penitents and roaming flagellants.[5][6] The advent of the microscope and the germ theory and the discoveries by scientists and doctors such as Louis Pasteur and Robert Koch that disease could be caused by micro-organisms changed the way we thought about disease and led to the development of the disciplines of bacteriology and preventive public health.[7]
Louis Pasteur was a French chemist and bacteriologist whose experiments supported the new germ theory of disease, countering the prevailing view of spontaneous generation of disease. He showed that the souring of wine and beer were due to micro-organisms, which he called ‘ferments’, and which were actually various types of cocci and bacilli, and proposed the idea that such micro-organisms could cause disease in humans. In 1863 he refined the process of pasteurisation of wine and later applied it to milk, heating milk to kill organisms to prevent the spread of diseases such as tuberculosis and typhoid. Pasteur also worked in developing vaccines, he successfully demonstrated the effectiveness of the anthrax vaccine in preventing anthrax and in 1885 developed the rabies vaccine.[3][7][8]
Robert Koch was a German physician who after serving in the Franco-Prussian War worked in the Royal Prussian Institute for Infectious Diseases in Berlin (now the Robert Koch Institute) and was instrumental in discovering the causes of many infectious diseases. In 1879 he published that traumatic wound infections were caused by bacteria. In 1882 he discovered the causative organism of tuberculosis, and of cholera in the following year. He showed that the anthrax bacillus, which was previously discovered by Franz Pollender, under certain conditions formed spores which could last for many years in soil and cause re-emergence of infection in animals. Koch also developed methods for staining histological specimens with dyes and the use of gelatine and later blood-serum and agar-agar in developing culture mediums that were more effective than the broth mediums. His students and his rivals used his methods to discover the causative organisms of many other diseases including typhoid, diphtheria, tetanus, leprosy, gonorrhoea, syphilis, and coccal infections such as pneumonia and meningitis.[3][7][8] Koch was a pupil of Jakob Henle, also a German physician and pathologist, and together they developed the Henle-Koch postulates which are required for proof that a particular micro-organism causes a particular disease.[9]
Early in 1894 bubonic plague broke out in Canton and Hong Kong, the start of the third great plague pandemic. Two bacteriologists immediately began working independently from one another to isolate and culture the causative organism of the plague; Shibasaburo Kitasato, a previous pupil of Robert Koch, and Alexandre Yersin, from the Pasteur Institute.[10][11][12]
On June 12 a Japanese team of researchers led jointly by Shibasaburo Kitasato and Aoyama Tanemichi arrived in Hong Kong to try to identify the organism responsible for the plague. Kitasato was a renowned Japanese bacteriologist who worked with Emil von Behring and Robert Koch in Berlin where they developed antitoxins for tetanus and diphtheria.[11][12] James Lowson, the British physician in charge of the Hong Kong plague emergency, set up Kitasato’s team with a well furnished laboratory in Kennedy Town Hospital. Kitasato found bacilli in the bubo pus, blood and organs of a plague victim who had died. He cultured the bacillus on broth culture and inoculated mice and other animals who died with the same bacilli in their blood.[13] On June 14 Kitasato informed Lowson that he had found the likely plague bacteria and Lowson immediately cabled The Lancet who published Kitasato’s findings in an editorial the next week, and his full research report in August, with great admiration from the Hong Kong and Japanese governments.[11]

Alexandre Yersin, a Franco-Swiss physician, was the assistant of Emile Roux, director of the Pasteur Institute, a fellow colleague of Pasteur, and a member of the Pasteur Institute, a Pastorien. He had also studied under Robert Koch in Germany and in 1888 was awarded the Paris Medical Faculty bronze medal for his work on animal tuberculosis and the diphtheria exotoxin. In 1890 Yersin decided to leave his work at the Pasteur Institute to go to French Vietnam, earning his passage on the way as a ship’s physician for the Messageries Maritimes company.[14] He arrived in Saigon and joined the French colonial health service as a missionary doctor. After plague had broken out in Hong Kong in 1894 he was asked by the Pasteur Institute to leave Vietnam and go to Hong Kong to try to isolate the plague organism, taking with him a microscope and an incubator as his only equipment. Yersin arrived in Hong Kong in June 1984 three days after Kitasato, Kitasato was already at work, but with a sophisticated laboratory and a staff of twenty or so.[10][12][14][15]
Yersin was not able to either obtain hospital laboratory facilities or to be able to work alongside Kitasato, and instead set up a rudimentary laboratory in a hut near the Hong Kong Hospital and had to make do with working on hospital patient corpses. A week into his stay, one of the mice he had inoculated with pus taken from a bubo on a corpse, died. Its spleen contained “very small, stocky, round tipped bacilli which could be stained only with difficulty”. In the following week he successfully obtained pure cultures of the bacillus on medium. He also demonstrated for the first time that the same bacillus was present in the rat as well as in the human disease, indicating its possible means of transmission.[11][12][14][15]
During June 1984 both Kitasato and Yersin announced isolation and culture of the plague bacillus. Although Kitasato was initially credited with the discovery for some years, it is now considered Yersin’s description of the bacillus to have been the more accurate. Yersin’s experiments satisfied Koch’s postulates for plague infection, his descriptions of the bacillus were more accurate and consistent than Kitasato’s, and he more accurately described the aniline dye and non-Gram staining of the bacillus. In addition, Kitasato’s cultures were probably contaminated by a gram-positive pneumococcus that was the cause of a secondary septicaemia in plague patients.[10][13][15][16] Yersin published his report in the Annales de l’Institut Pasteur with a paper titled La peste bubonique á Hong Kong and the bacillus was named Bacterium pestis. A few months after his return to France, Yersin was awarded the Légion d’honneur by Delcasse, the French Minister of Colonies.[14][15]
Following is a description of the plague from his 1894 paper :
“The onset is rapid, with an incubation of 4½ to 6 days. The patient is prostrated. Abruptly, a high fever sets in, often accompanied by delirium. On the very first day a discrete bubo usually appears. In 75% of the cases it is located in the inguinal region, in 10% of the cases in the axillary region, and occasionally at the back of the neck and in other regions. The nodule rapidly reaches the size of an egg. Death occurs after 48 hours and often sooner. If the patient manages to survive 5 to 6 days, the prognosis is better, the bubo softens and one can operate to aspirate the pus. In a few cases, the bubo does not form, and one will note in such cases haemorrhages in the mucous membranes or petechial spots on the skin. Mortality is high; 95% in the hospitals.”[13]
While working on the bacillus Yersin had also noticed that the streets of Hong Kong were littered with dead rats. It had been observed throughout history, such as by Avicenna in Persia in the 11th century and by Nathaniel Hodges in 1665 in his work Loimographia, or an historical Account of the Plague in London in 1665, With precautionary Directions against the like Contagion that a plague of dead rats often heralded an epidemic in people.[10] It is now known that epizootic infection in rats precedes a human epidemic of plague and that rats have just as great a mortality as humans. When all the rats die the fleas actively seek new hosts, people and their domestic animals being the closest, thus propagating an epidemic. Yersin suspected that there was a connection between rats, the bacillus, and epidemics, but didn’t know how the rats transmitted the bacillus if they were the vector.[10][17]
In 1895 on his return to the Pasteur Institute, Yersin, in collaboration with Amedee Borrel and Albert Calmette, both Pastorien bacteriologists, began experimenting with an anti-plague serum and in 1897 Yersin went to back Bombay to continue trialling his antiserum, although he had poor success as only half of his patients survived.[14] Yersin had a falling out with the local authorities and left Bombay to return to Nha Trang in Vietnam. In 1902 he founded a medical school in Hanoi and in 1924 was made Honorary Inspector General for Indochina’s Pasteur Institutes. Yersin died in his home in Nha Trang in 1943 where his grave is honoured as that of a national hero.[14][15] In 1900 the bacillus, Bacterium pestis, was renamed Bacillus pestis, then renamed again in 1923 as Pasteurella pestis after Pasteur. In 1970 the bacillus was reclassified as a different genus to Pasteurella and was renamed Yersinia pestis.[13][16]
Yersin’s position in Bombay was taken over by Paul-Louis Simond, a young doctor in the French Navy, and like Yersin, was a fellow Pastorien. Simond earned his medical doctorate in 1887 and was awarded the Godard prize for his dissertation on leprosy in French Guyana. Simond joined the French Naval Medical Corps, the Médecin de première class, and was posted to French Guyana and the Far East, until in 1895 he returned to Paris and joined the Pasteur Institute to study the biology of coccidians and Plasmodium protozoa. In 1897 he was sent to India by the Institute to replace Yersin and continue his work on the antiserum for plague.[18][19]

In Bombay, Simond continued with Yersin’s hypothesis about there being a vector for the bacillus. He noticed tiny fluid filled vesicles, phlyctene precoce, on the legs and feet of plague patients which he found to be swarming with plague bacilli.[10][18] He considered these to be the primary lesion preceding formation of a bubo and that it may be caused by an insect bite, and in particular, the flea. He also noted, like Yersin in Hong Kong, that the streets of Bombay were littered with dead rats. He wrote as one of his observations:
“On the rats captured alive, and on the rats which had just died, the fleas were thicker than I have ever seen them… We have to assume there must be an intermediary between a dead rat and a human. This intermediary might be the flea.”[10]
In 1898 in Karachi Simond, using a very simple experiment with an infected rat and its fleas and a healthy rat, showed that the bacillus was transmitted by the fleas, and that the brown sewer rats were the main host of the bacillus. He published his experiment and findings in the Annales de l’Institut Pasteur with his paper La Propagation de la Peste and was awarded the Barbier Prize from the French Academy of Medicine for his work. Unfortunately Simond’s theory and his experiments about a flea vector were met with great scorn from the European medical authorities despite evidence for some decades that insects were known to be a vector for several epidemic diseases such as filariasis and yellow fever. In 1901 Simond was awarded the Légion d’honneur in Paris and went on to study yellow fever in Brazil but was not given credit for his flea discovery until many years later.[15][18][19]
In 1906 Simond became professor at the Graduate School of the French Colonial Health Service and continued his work on the prevention of mosquito transmission of yellow fever and the development of a vaccine for typhus. In 1913 he became a corresponding member of the French Society of Biology for his passion and work with classifying orchids in Indochina. During the first world war he was Director of the Colonial Health Service and Inspector of Hygiene and Health Services in Indochina. From 1919 he worked in public health and prevention of tuberculosis in Valence where he died in 1947.[19]
In 1902 in the Sydney outbreak of plague, John Ashburton-Thompson, the chief medical officer, embraced the hypothesis of the rat flea as the plague vector and identified the fleas Pulex pallidus and Pulex fasciatus as the main vectors in the outbreak.[20] He confirmed that there was a close association between rats and plague in humans and that an epizootic in rats always preceded an epidemic, and also made the observation that rats during a plague epizootic harboured more fleas than at other times.[21]
The flea vector hypothesis was also confirmed by Masanori Ogata in 1898, G. Zirolia in 1902, and J-C. Gauthier and A. Raybaud in 1902 and 1903 in similar experiments to Simond’s. In 1903 Nathaniel Charles Rothschild, a British entomologist, identified specimens of the Indian rat flea found during a plague outbreak in Egypt and Sudan as Pulex cheopis (named by Rothschild after the pharaoh Cheops, and renamed Xenopsylla cheopis by Rothschild and Karl Jordan in 1911) which was later considered to be identical to the Pulex pallidus in the plague outbreaks that occurred in Sydney and other places throughout Australia.[17][20][22]
Around 1900, Waldemar Haffkine, a Russian physician working for the Indian government during the epidemic, developed a killed plague vaccine. This work was continued in the 1920’s and 1930’s by Albert Calmette, Kiyoshu Shiga, and Alexandre Besredka who developed reasonably effective killed vaccines, and by George Girard and Jean-Marie Robic who developed a live vaccine from a non-virulent strain of the bacillus.[3][7][15]
Plague continued on as a world pandemic until 1959 and in that time many physicians and scientists made important contributions to our knowledge of plague. The early discoveries in particular by two French physicians, Alexandre Yersin and Paul- Louis Simond, gave medicine the beginnings of a long sought after insight into the bubonic plague – the nature of the bacterium that caused it, the relationship between the bacillus and the primary hosts, the urban and sewer rats, and its transmission to humans by the bite of the rat flea.
Notes
The Three Great Pandemics
- Centers for Disease Control and Prevention. Emergency Preparedness and Response: Bioterrorism – Agents/Diseases, accessed on 6.11.11.
- Achtman M, Zurth K, Morelli G, Torrea G, Guiyoule A, Carniel E. Yersinia pestis, the cause of plague, is a recently emerged clone of Yersinia pseudotuberculosis. Proc Natl Acad Sci 1999; 96 (24): 14043- 14048, accessed on 3.11.11.
- Echenberg M. Plague Ports. New York; New York University Press, 2007.
- Marriott E. Plague. New York: Metropolitan Books – Henry Holt & Co, 2003.
- Gage KL, Kosoy MY. Natural history of plague: perspectives from more than a century of research. Ann Rev Entomol 2005; 50: 505-528, accessed on 15.11.11.
- Drancourt M, Roux V, Dang LV, Tran-Hung L, Castex D, Chenal-Francisque V, Ogata H, Fournier P-E, Crubezy E, Raoult D. Genotyping Orientalis-like Yersinia pestis, and plague pandemics. Emerging Inf Dis 2004; 10 (9): 1585-1592, accessed on 3.11.11
- Raoult D, Drancourt M. Yersinia Pestis and Plague. University of Marseille. 2006, accessed on 3.11.11.
- Dobson M. Disease: The Extraordinary Stories Behind History’s Deadliest Killers. Quercus: London, 2007.
- Porter S. The Great Plague. Phoenix Mill, Gloucestershire; Sutton Publishing, 1999.
- Gratz N. Rodent Reservoirs & Flea Vectors of Natural Foci of Plague. In : WHO. Plague Manual: Epidemiology, Distribution, Surveillance and Control. 2011. WHO/CDS/CSR/EDC/99.2, accessed on 19.11.11.
- Butler T. Plague and Other Yersinia Infections. New York: Plenum Medical Book Company, 1983.
- Rosen W. Justinian’s Flea: The First Great Plague and the End of the Roman Empire. New York: Viking Penguin, 2007.
- Gottfried RS. The Black Death. London: Robert Hale Ltd, 1983.
- Halsall P. Medieval Sourcebook: Procopius: The Plague, 542. 1998, accessed on 19.11.11.
- Tikhomirov E. Epidemiology and Distribution of Plague. In : WHO. Plague Manual: Epidemiology, Distribution, Surveillance and Control. 2011. WHO/CDS/CSR/EDC/99.2, accessed on 10.11.11.
- Morony MG. “For Whom Does the Writer Write ?” The First Bubonic Plague Pandemic According to Syriac Sources. In : Little LK. Plague and the End of Antiquity: The Pandemic of 541-750. Cambridge: Cambridge University Press, 2007.
- Zeigler P. The Black Death. Godalming, Surrey: Bramley Books, 1969.
- Garrison F H. An Introduction to the History of Medicine. Philadelphia & London: W B Saunders & Co., 1921.
- Schreiber W, Mathys FK. Infectio: Infectious Diseases in the History of Medicine. Basle: F. Hoffman – La Roche & Co, 1987.
- Nohl J. The Black Death: A Chronicle of the Plague. (Translated by CH Clarke). London: George Allen & Unwin, 1926.
- Damen M. History and Civilisation: Section 6: The Black Death. 2010. [On-line], accessed on 1.4.12.
- Mackowiak PA, Sehdev PS. The origin of quarantine. Clin Infect Dis 2002; 35 (9): 1071-1072, accessed on 17.11.11
- Gregg CT. Plague: An Ancient Disease in the Twentieth Century. Revised edition. Albuquerque; University of New Mexico Press, 1985.
- Archives de l’ Institut Pasteur. Alexandre Yersin (1863-1943, accessed on 24.11.10.
- Archives de l’ Institut Pasteur. Paul-Louis Simond (1858-1947), accessed on 27.10.11.
- Curson PH. Times of Crisis: Epidemics in Sydney 1788-1900. Sydney: Sydney University Press, 1985.
- Perry RD, Fetherston JD. Yersinia pestis – etiologic agent of plague. Clin Microbiol Rev 1997; 10 (1): 35- 66, accessed on 2.4.12.
- WHO. Zoonotic Infections – Plague. 2012, accessed on 2.4.12.
The Discoveries of the Plague Bacillus and Its Vector
- Wigham JT. War, famine and pestilence. Irish J Med Sci 1939; 6th series, No. 158: 49-58.
- Kiple KF. Purveyors of pestilence, urbanism, war trade and imperialism. In : Kiple KF (Editor). Plague, Pox & Pestilence. London: Weidenfeld & Nicolson, 1997.
- Singer C, Underwood EA. A Short History of Medicine. 2nd edition. Oxford: Oxford University Press, 1962
- Centers for Disease Control and Prevention. Emergency Preparedness and Response: Bioterrorism – Agents/Diseases, accessed on 6.11.11.
- Zeigler P. The Black Death. Godalming, Surrey: Bramley Books, 1969.
- Schreiber W, Mathys FK. Infectio: Infectious Diseases in the History of Medicine. Basle; F. Hoffman – La Roche & Co, 1987.
- Garrison F H. An Introduction to the History of Medicine. Philadelphia & London: W B Saunders & Co., 1921.
- Porter R. Medical science. In : Porter R (editor). The Cambridge Illustrated History of Medicine. Cambridge: Cambridge University Press, 1996.
- Evans AS. Causation of disease: the Henle-Koch postulates revisited. Yale J Biol Med 1976; 49: 175-195, accessed on 24.4.12.
- Marriott E. Plague. New York: Metropolitan Books – Henry Holt & Co, 2003.
- Echenberg M. Plague Ports. New York; New York University Press, 2007.
- Wills C. Plagues: Their origin, History and Future. London: Harper Collins Publishers, 1996.
- Butler T. Plague and Other Yersinia Infections. New York: Plenum Medical Book Company, 1983.
- Archives de l’Institut Pasteur. Alexandre Yersin (1863-1943), accessed on 24.11.10.
- Association Amicale Santé Navale et d’outre Mer. The Plague accessed on 24.11.10.
- Perry RD, Fetherston JD. Yersinia pestis – etiologic agent of plague. Clin Microbiol Rev 1997; 10 (1): 35- 66, accessed on 2.4.12.
- Dobson M. Disease: The Extraordinary Stories Behind History’s Deadliest Killers. Quercus: London, 2007.
- Simond M, Godley ML, Mouriquand PDE. Paul-Louis Simond and his discovery of the plague transmission by rat fleas: a centenary. J Roy Soc Med 1998; 91: 101-104 , accessed on 24.11.10.
- Archives de l’Institut Pasteur. Paul-Louis Simond (1858-1947), accessed on 27.10.11.
- Experiments upon the transmission of plague by fleas. (No authors listed) J Hyg 1906; 6 (4): 425-434.2, accessed on 24.11.10.
- Curson PH. Times of Crisis: Epidemics in Sydney 1788-1900. Sydney: Sydney University Press, 1985.
Originally published by the Journal of Military and Veterans’ Health (20:2, April 2012 and 20:3, August 2012) under the terms of a Creative Commons Attribution 4.0 International license.