

Photo Credit EMSL, Creative Commons

Edited by Matthew A. McIntosh / 02.22.2018
Historian
Brewminate Editor-in-Chief
1 – Introduction to Consciousness
1.1 – Introduction
1.1.1 – Philosophy of Consciousness
Despite the difficulty in coming to a definition, many philosophers believe that there is a broadly shared underlying intuition about what consciousness is. Philosophers since the time of Descartes and Locke have struggled to comprehend the nature of consciousness and pin down its essential properties. Issues of concern in the philosophy of consciousness include the following: whether consciousness can ever be explained mechanistically; whether non-human consciousness exists, and if so, how it can be recognized; how consciousness relates to language; whether consciousness can be understood in a way that does not require a dualistic distinction between mental and physical states or properties; and whether it may ever be possible for computers or robots to be conscious.
1.1.2 – The Mind-Body Problem
The mind-body problem is essentially the problem of consciousness; roughly speaking, it is the question of how mental experiences arise from a physical entity. How are our mental states, beliefs, actions, and thinking related to our physical states, bodily functions, and external events, given that the body is physical and the mind is non-physical?
The first and most important philosopher to address this conundrum was René Descartes in the 17th century, and his answer was termed Cartesian dualism. The explanation behind Cartesian dualism is that consciousness resides within an immaterial domain he called res cogitans (the realm of thought), in contrast to the domain of material things, which he called res extensa (the realm of extension). He suggested that the interaction between these two domains occurs inside the brain. He further suggested the pineal glad as the point of interaction, but was later challenged several times on this claim. These challenges sparked some key initial research on consciousness, which we will discuss shortly.
1.1.3 – Early Ideas on Consciousness
For over 2000 years, questions surrounding human consciousness—such as how the everyday inner workings of our brains give rise to a single cohesive reality and a sense of an individual self—have been baffling philosophers from Plato to Descartes. Descartes, as previously mentioned, is noted for his dualist theory of consciousness, in which the physical body is separate from the immaterial mind. He also gave us the most famous summary of human consciousness: “I think, therefore I am.”
The historical materialism of Karl Marx rejects the mind-body dichotomy, and holds that consciousness is engendered by the material contingencies of one’s environment. John Locke, another early philosopher, claimed that consciousness, and therefore personal identity, are independent of all substances. He pointed out that there is no reason to assume that consciousness is tied to any particular body or mind, or that consciousness cannot be transferred from one body or mind to another.
American psychologist William James compared consciousness to a stream—unbroken and continuous despite constant shifts and changes. While the focus of much of the research in psychology shifted to purely observable behaviors during the first half of the twentieth century, research on human consciousness has grown tremendously since the 1950s.
1.1.4 – Current Research on Consciousness

Prefrontal cortex: This image shows the location of the prefrontal cortex, an area of the brain heavily involved in consciousness.
Today, the primary focus of consciousness research is on understanding what consciousness means both biologically and psychologically. It questions what it means for information to be present in consciousness, and seeks to determine the neural and psychological correlates of consciousness. Issues of interest include phenomena such as perception, subliminal perception, blindsight, anosognosia, brainwaves during sleep, and altered states of consciousness produced by psychoactive drugs or spiritual or meditative techniques.
The majority of experimental studies assess consciousness by asking human subjects for a verbal report of their experiences. However, in order to confirm the significance of these verbal reports, scientists must compare them to the activity that simultaneously takes place in the brain—that is, they must look for the neural correlates of consciousness. The hope is to find that observable activity in a particular part of the brain, or a particular pattern of global brain activity, will be strongly predictive of conscious awareness. Several brain-imaging techniques, such as EEG and fMRI scans, have been used for physical measures of brain activity in these studies.
Higher brain areas are more widely accepted as necessary for consciousness to occur, especially the prefrontal cortex, which is involved in a range of higher cognitive functions collectively known as executive functions.
1.2 – A History of Theories of Consciousness
Theories of consciousness include developmental, cultural, neural, computational, and moral perspectives.
1.2.1 – Mayan and Incan Theories of Consciousness
First appearing in the historical records of the ancient Mayan and Incan civilizations, various theories of multiple levels of consciousness have pervaded spiritual, psychological, medical, and moral speculations in both Eastern and Western cultures. Consciousness can be defined as human awareness to both internal and external stimuli. Because of occasional and sometimes substantial overlap between hypotheses, there have recently been attempts to combine perspectives to form new models that integrate components of separate viewpoints.
The Ancient Mayans were among the first to propose an organized sense of each level of consciousness, its purpose, and its temporal connection to humankind. Because consciousness incorporates stimuli from the environment as well as internal stimuli, the Mayans believed it to be the most basic form of existence, capable of evolution. The Incas, however, considered consciousness a progression not only of awareness but of concern for others as well.
1.2.2 – John Locke on Consciousness
John Locke, a 17th-century philosopher, was one of the first to speak and write on consciousness. He believed that our identity was tied to our consciousness, which he essentially defined as what passes through a man’s mind, or memories. He also asserted that our consciousness is not tied to our physical bodies, and that it can survive even after our physical bodies die. In fact, Locke held that consciousness could be transferred from one soul to another.
1.2.3 – René Descartes on Consciousness
René Descartes also addressed the idea of consciousness in the 17th century. He set out to answer the question of how it is possible that our consciousness, a non-physical thing, can come from our bodies, a physical thing. The explanation he came up with was called Cartesian dualism; in short, consciousness resides within an immaterial domain he called res cogitans (the realm of thought), in contrast to the domain of material things, which he called res extensa (the realm of extension). He suggested that the interaction between these two domains occurs inside the brain.
1.2.4 – Sigmund Freud on Consciousness
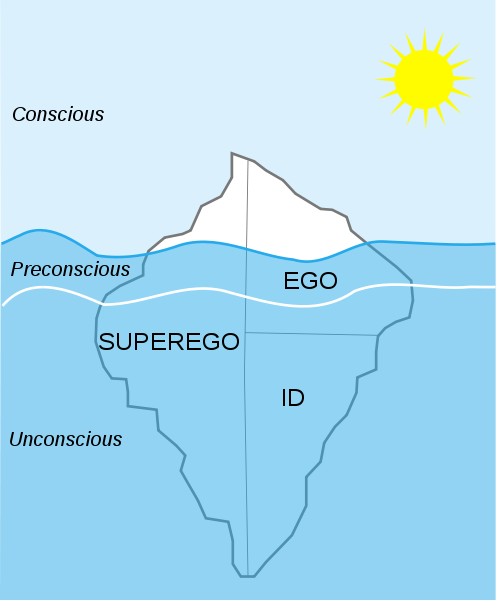
Freud’s levels of consciousness: This figure illustrates the respective levels of the id, ego, and superego. The part above water is known as the conscious level; the top level of waves just below the surface and above the white line is the preconscious level; and the bottom level is the unconscious.
While Eastern perspectives on consciousness have remained relatively stable over the centuries, fluctuations in theory have come to define the Western perspective. One of the most popular Western theories is that of Sigmund Freud, medical doctor and father of psychoanalytic theory. Freud divided human consciousness into three levels of awareness: the conscious, preconscious, and unconscious. Each of these levels corresponds and overlaps with Freud’s ideas of the id, ego, and superego. The conscious level consists of all the things we are aware of, including things we know about ourselves and our surroundings. The preconscious consists of things we could pay conscious attention to if we so desired, and is where many memories are stored for easy retrieval. Freud saw the preconscious as comprised of thoughts that are unconscious at the particular moment in question, but that are not repressed and are therefore available for recall and easily capable of becoming conscious (for example, the tip-of-the-tongue effect). The unconscious consists of things that are outside of conscious awareness, including many memories, thoughts, and urges of which we are not aware. Much of what is stored in the unconscious is thought to be unpleasant or conflicting; for example, sexual impulses that are deemed unacceptable. While these elements are stored out of our awareness, they are nevertheless thought to influence our behavior.
1.2.5 – Modern Theories of Consciousness
While Freud’s theory remains one of the best known, various schools in the field of psychology have developed their own perspectives, which we will explore below. It is important to note that these perspectives are not necessarily mutually exclusive, just different approaches to the same questions.
1.2.6 – Developmental Psychology on Consciousness
Developmental psychologists view consciousness not as a single entity, but as a developmental process with potential higher stages of cognitive, moral, and spiritual quality. They posit that consciousness changes over time, in quality and in degree: an infant’s consciousness is qualitatively different than a toddler’s, a teenager’s, or an adult’s. Abnormal development also affects consciousness, as do mental illnesses.
1.2.7 – Social Psychology on Consciousness
Social psychologists view consciousness as a product of cultural influence having little to do with the individual. For instance, because different cultures speak different languages, they also codify reality differently. That difference in codification leads to differences in the experience of reality, and therefore of consciousness. Language is the main mechanism for transmitting a mode of consciousness, and an analysis of language can to some extent reveal the mentality of people who speak that language.
1.2.8 – Neuropsychology on Consciousness
Neuropsychologists view consciousness as ingrained in neural systems and organic brain structures. A major part of the modern scientific literature on consciousness consists of studies that examine the relationship between the experiences reported by subjects and the activity that simultaneously takes place in their brains—that is, studies of the neural correlates of consciousness. The hope is to find activity in a particular part of the brain, or a particular pattern of global brain activity, that will be strongly predictive of conscious awareness. Several brain-imaging techniques, such as EEG and fMRI, have been used for physical measures of brain activity in these studies.
1.3 – Neural Underpinnings of Consciousness
The neural correlates of consciousness (NCC) refer to the relationship between the experiences reported by subjects and the activity that simultaneously takes place in their brains.
Consciousness is the awareness of the self, the environment, and the relationship between these two distinct worlds. From ancient philosophers to modern-day scientists, many people have struggled to understand, research, and document the processes involved in human consciousness. Thanks in large part to advances in medicine, science, and psychology, we have learned much about how states of consciousness are created. Current research studies the neural correlates of consciousness by examining experiences reported by subjects and recording the simultaneous activity that takes place in their brains. Researchers continue to search for brain activity or global brain patterns that can be predictive of conscious awareness.
1.3.1 – Neural Correlates of Consciousness (NCC)
The neural correlates of consciousness (NCC) refer to the relationship between the experiences reported by subjects and the activity that simultaneously takes place in their brains. The physical world is perceived by human consciousness through the senses, which funnel stimuli and information into the central nervous system, and eventually the brain. The brain is the major organ implicated in turning physical stimuli into thoughts and actions. The study of NCC seeks to link objective, observable, neural activity to subjective, unobservable, conscious phenomena. While discovering and characterizing neural correlates cannot offer its own theory of consciousness, the data and findings may one day lead to such a discovery.

Neural correlates of consciousness: The study of neural correlates of consciousness seeks to link activity within the brain to subjective human experiences in the physical world.
Neural networks have been found to have a large amount of redundancy and parallelism, such that activity in one set of neurons cannot necessarily be said to correlate with the same perception over time. Scientists believe it may be the case that every phenomenal, subjective state has its own neural correlate. Continued advances in the ability to stimulate or induce activity in certain brain regions or sets of neural networks will help scientists answer ever more complicated questions about the characteristics and commonalities among neural correlates.
1.3.2 – Neurobiology and Consciousness
The science of consciousness sets out to explain the precise relationship between subjective mental states and brain states, the relationship between the conscious mind and the electro-chemical interactions in the body. Progress in this arena has come from focusing on the body rather than the mind. In this context, the neuronal correlates of consciousness may be viewed as its causes, and consciousness may be thought of as a state-dependent property of some complex, adaptive, and highly interconnected biological system.
Most neurobiologists assume that the variables giving rise to consciousness are to be found at the neuronal level, governed by classical physics. More than ever before, neuroscientists are able to manipulate neurons using methods from molecular biology combined with state-of-the-art optical tools (e.g., Adamantidis et al., 2007). Neuronal analysis and brain imaging techniques have become so fine-grained that a rational understanding of consciousness is within reach.
1.3.3 – Dimensions and Neural Consciousness: Arousal and Content
Neuronal consciousness is often described as involving two distinct dimensions: arousal and content. In order for the brain to be conscious of any type of content, it must be in a high state of arousal. While awake and dreaming states are fundamentally different states of consciousness, they are both high-arousal, and thus allow for perception. Sleep is just one of the many types of consciousness we can experience and comprises several states of consciousness itself. Consciousness can also be phenomenal, such as our experiences in real time, or access, such as recalling a state of being or feeling.
1.3.4 – Brain Areas Implicated in Consciousness
Another idea that has drawn attention for several decades is that consciousness is associated with high-frequency (gamma band) oscillations in brain activity. This idea arose from proposals in the 1980s, by Christof von der Malsburg and Wolf Singer, that gamma oscillations may link information represented in different parts of the brain into a unified experience.
Several studies have demonstrated that activity in primary sensory areas of the brain is not sufficient to produce consciousness: it is possible for subjects to report a lack of awareness even when areas such as the primary visual cortex show clear electrical responses to a stimulus. Higher brain areas are seen as more promising, especially the prefrontal cortex, which is involved in a range of executive (higher-order) functions. There is substantial evidence that a “top-down” flow of neural activity (i.e., activity propagating from the frontal cortex to sensory areas) is more predictive of consciousness than a “bottom-up” flow of activity. The prefrontal cortex is not the only candidate area, however: studies have shown that visually responsive neurons in parts of the temporal lobe reflect the visual perception in the situation when conflicting visual images are presented to different eyes.
1.3.5 – Brain Imaging and Consciousness
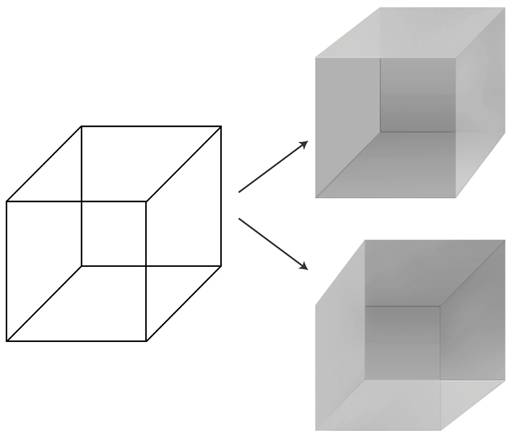
The Necker cube: The Necker cube is a popular visual stimulus used to study differences in human visual perception. It is possible to perceive the front of the cube at two different angles.
One popular theory implicates different patterns of brain waves in producing different states of consciousness. Researchers can record brain waves, or tracings of electrical activity within the brain, using an electroencephalograph (EEG) and placing electrodes on the scalp. The four types of brain waves (alpha, beta, theta, and delta) each correspond with one mental state (relaxed, alert, lightly asleep, and deeply asleep, respectively).
Functional magnetic resonance imaging (fMRI) scans, can also be used to measure physical activity in the brain that correlates with different conscious states and perceptions. The ease in which visual perceptions can be manipulated in time and space has made visual studies, such as the Necker cube, one of the most preferred modalities for studying the neural correlates of consciousness. These studies take a seemingly simple and unambiguous visual stimulus and record differences in its subjective perception by a study participant. The cube, for instance, is 12 basic lines that can be interpreted in two different depths, creating a visual illusion. Scientists are interested in locating which neural correlates lead to differing mental interpretations.
2 – Sleep and Dreaming
2.1 – Introduction to Sleep
Most adults need seven to nine hours of sleep to recuperate from physical exertion, as well as to consolidate learning and memory.
2.1.1 – Why Do We Need Sleep?
Along with food and water, sleep is one of the human body’s most important physiological needs—we cannot live without it. Extended sleeplessness (i.e., lack of sleep for longer than a few days) has severe psychological and physical effects. Research on rats has found that a week of no sleep leads to loss of immune function, and two weeks of no sleep leads to death.
Despite its clear importance to psychological and physiological functioning, researchers have struggled for centuries to answer the question of why we sleep. On the surface, we know that sleep helps our body recuperate from a day’s physical exertions. It also aids in recovery from illnesses and infections. We also know that extended sleeplessness can lead to hallucinations, delusions, loss of immune function, and in extreme cases, death. Modern research has also uncovered that sleep has a major role in maintaining our mental and emotional health.
Recently, neuroscientists have learned that at least one vital function of sleep is related to learning and memory. New findings suggest that sleep plays a critical role in flagging and storing important memories, both intellectual and physical, and perhaps in making subtle connections that were invisible during waking hours.
Though scientists are still learning about the concept of basal sleep need (just how much sleep we need), research has demonstrated that sleeping too little can inhibit your productivity and your ability to remember and consolidate information. Lack of sleep can also lead to serious health consequences, jeopardizing individual safety and the safety of others.
For example, sleep deprivation is related to:
- higher rates of motor vehicle accidents;
- higher BMI, an increased likelihood of obesity, and increased risk of diabetes and heart problems;
- higher risk for depression and substance abuse;
- decreased attention, slower reaction times, and the inability to remember new information.
When we do not sleep enough, we accumulate a sleep debt. Sleep debt occurs as the result of not getting enough sleep, and a large debt causes mental, emotional, and physical fatigue. Sleep debt results in diminished abilities to perform high-level cognitive functions.
2.1.2 – How Much Sleep Do We Need?
The amount of sleep we need varies depending on multiple factors including age, physical condition, psychological condition, and energy exertion. Therefore, sleep requirements depend entirely on the individual. Just like any other human characteristic, the amount of sleep people need to function best differs among individuals, even those of the same age and gender. For example, a pregnant woman will need more sleep than a healthy woman of the same age, an adult with a cold will need more sleep than one who is well, and an individual with depression may require more sleep than a non-depressed person.
Though there is no magic sleep number, there are general rules for how much sleep certain age groups need. For instance, children need more sleep per day in order to develop and function properly: up to 18 hours for newborn babies, with a declining rate as a child ages. A newborn baby spends almost 9 hours a day in REM sleep. By the age of five, only slightly over two hours is spent in REM. Studies show that young children need about 10 to 11 hours of sleep, adolescents need between 8.5 and 9.25, and adults generally need between 7 and 9 hours.
2.1.3 – Effects of Sleep Deprivation
Research has uncovered a number of ways that a lack of sleep affects our well-being. Sleep deprivation negatively affects brain chemistry, growth, healing, attention, memory, and the ability to operate machinery, among other things. Sleep deprivation can cause both physical and mental illness, such as diabetes, depression, and psychosis, and in extreme cases, it can cause hallucinations and death.
2.1.3.1 – Sleep Deprivation on the Brain and Body
Numerous studies have demonstrated that sleep deprivation can adversely affect brain growth and cognitive functions. fMRI studies performed on sleep-deprived subjects show that regions of the brain’s prefrontal cortex, an area that supports mental faculties such as working memory and logical reasoning, displayed more activity in sleepier subjects. The results implied that sleepier subjects had to work harder than well-rested subjects to accomplish the same task, indicating the need to compensate for adverse effects caused by sleep deprivation.
The link between sleep deprivation and psychosis has been well-documented. In 2007, a study at Harvard Medical School and the University of California at Berkeley revealed, using MRI scans, that sleep deprivation causes the brain to become incapable of putting an emotional event into the proper perspective and incapable of making a controlled, suitable response to the event.
The negative effects of sleep deprivation on alertness and cognitive performance suggest decreases in brain activity and function, primarily in the thalamus, a structure involved in alertness and attention, and in the prefrontal cortex, a region sub-serving alertness, attention, and higher-order cognitive processes.
Sleep deprivation has also been found to inhibit stress reactions, body functions such as digestion, the immune system, mood, sex, and energy usage, while also suppressing growth hormones. Sleep deprivation has also been shown to slow the healing process, and has been implicated in weight gain and type-2 diabetes.
2.2 – Circadian Rhythms
2.2.1 – Introduction
Circadian rhythms are physical, mental, and behavioral changes that respond to light and darkness and are important in determining human sleep patterns.
Circadian rhythms are physical, mental, and behavioral changes that follow an approximate 24-hour cycle, responding primarily to light and darkness in an organism’s environment. Circadian rhythms are found in most living things, including animals, plants, and many tiny microbes. These rhythms can influence sleep-wake cycles, hormone release, body temperature, and other important bodily functions. The study of circadian rhythms (and biological temporal rhythms in general) is called chronobiology.
2.2.2 – Circadian Rhythms and the Suprachiasmatic Nucleus

The suprachasmatic nucleus: The SCN contains about 20,000 nerve cells, and is located in the hypothalamus, above the optic nerves.
Circadian rhythms are important in determining human sleep patterns. The body’s master clock, or the suprachiasmatic nucleus (SCN), controls the production of melatonin, a hormone that makes you sleepy. The SCN is a small group of brain cells located in the hypothalamus that controls the circadian cycles and influences many physiological and behavioral rhythms occurring over a 24-hour period, including the sleep/wake cycle. The circadian pacemaker, located in the SCN, regulates the timing and consolidation of the sleep-wake cycle, while sleep-wake homeostasis governs the accumulation of sleep debt and sleep recovery. Destruction of the SCN results in the complete absence of a regular sleep-wake rhythm.
2.2.3 – The Effect of Light on Circadian Rhythms
Circadian rhythms are maintained by individual organisms, and their length varies somewhat between individuals. Therefore, they must be reset, either continually or repeatedly, to synchronize with nature’s cycle. In order to maintain synchronization (a.k.a. entrainment ) to a 24-hour cycle, external factors must play some role; of these factors, light exposure to the eyes is the strongest.
The SCN receives information about light through the eyes. The retina of the eye contains photoreceptors (rods for seeing at night, and cones for distinguishing colors), which are used for conventional vision. But the retina also contains specialized ganglion cells, which are photosensitive and project directly to the SCN, where they help in the entrainment of this master circadian clock.
The mechanisms by which light affects entrainment are not yet fully known. However, studies have shown that timing of light exposure, the length of light exposure, and the intensity/wavelength of light all influence entrainment and circadian rhythms.
2.2.4 – Circadian Rhythms and Sleep

Circadian rhythms influence sleep: Circadian rhythms have a hand in determining when we are alert and when we become sleepy.
Our internal circadian pacemakers regulate the timing and duration of sleepiness and wakefulness throughout the day. The circadian rhythm falls and rises at different times of the day; in fact, numerous studies have demonstrated that human circadian rhythms in many measures of performance and physiological activity actually have a 2-peak daily (circasemidian) pattern. A typical adult will experience the strongest desire to sleep in the pre-dawn hours (around 2:00 a.m. to 4:00 a.m.) and in the early afternoon (around 1:00 p.m. to 3:00 p.m.). This frame may be slightly different depending on whether you are a “morning person” or a “night person.” The sleepiness we experience during these circadian dips will be less intense if we have had sufficient sleep, and more intense when we are sleep deprived. The circadian rhythm also causes us to feel more alert at certain points of the day, even if we have been awake for hours.
When we have been awake for an extended period of time, sleep-wake homeostasis tells us that the need for sleep is accumulating, and staying awake becomes more difficult.
2.2.5 – Segmented Sleep
Segmented sleep, also known as interrupted or divided sleep, is a multiphasic sleep pattern in which two or more periods of sleep are punctuated by periods of wakefulness. Along with a nap at mid-day, it has been argued that this is the natural pattern of human sleep. In fact, some scientists believe that maintenance of this sleep pattern is important in regulating stress.
Roger Ekirch, a historian who has researched segmented sleep extensively, argues that segmented sleep was the dominant form of human sleep before the Industrial Revolution. Circadian rhythms, as we’ve just discussed, are heavily influenced by light. Ekirch suggests that it is due to the modern use of electric lighting (computers, cell phones, office lights) that most modern humans do not practice
segmented sleep.
In one experiment on segmented sleep, researchers had eight healthy men confined to a room for fourteen hours of darkness every day for a month. At first the participants slept for about eleven hours, presumably making up for their sleep debt. After that the subjects began to sleep much as people in pre-industrial times did. They would sleep for about four hours, wake up for two to three hours, then go back to bed for another four hours. They also took about two hours to fall asleep. Together, these results imply that segmented sleep is indeed our natural sleep rhythm.
2.3 – Stages of Sleep
Sleep proceeds through multiple cycles of non-REM (3 stages) and REM per night, with each full cycle lasting between 90 and 110 minutes.
In mammals, the overall sleep cycle is comprised of two broad alternating cycles, REM (rapid eye movement), and NREM (non-rapid eye movement), which itself consists of three individual phases. (Note: REM is pronounced like a word [“rehm”], not as a series of initials. NREM, or non-REM, is pronounced phonetically as well, with the “N” standing alone [“en-rehm”].)
In electroencephalography, the REM phase of sleep is easily identified by its paradigmatic fast, small-amplitude waves. (Also typical are the rapid eye movements for which the REM phase is named.) For this reason REM sleep is sometimes also called “active sleep.” Many sleep experts think that these eye movements are in some way related to dreams. Sleep proceeds in cycles of REM and NREM, usually four or five per night. These cycles typically last between 90 and 110 minutes.
2.3.1 – Stages of NREM Sleep
2.3.1.1 – Stage 1 NREM (N1)
After a person falls asleep, he or she enters into what is known as stage 1 of non-REM sleep. This stage is sometimes referred to as somnolence, or drowsy sleep. Sudden twitches known as hypnic jerks are associated with this stage. The sleeper loses some muscle tone and most consciousness of the external environment. This stage lasts around ten minutes, during which a person can still be woken easily. A sleeper who has experienced only stage 1 NREM sleep may not even realize they slept at all. Stage 1 NREM is characterized by:
- slow, even breathing,
- regular heartbeat;
- lowered brain temperature.
2.3.1.2 – Stage 2 NREM (N2)
During this stage, muscular activity decreases, and conscious awareness of the external environment disappears. This stage occupies 45–55% of total sleep in adults. It is also characterized by:
- high-amplitude brain waves;
- sporadic short periods of increased activity;
- heightened sensitivity to sound stimuli (sleeper may wake up);
- slowed bodily functions (e.g., lower blood pressure; decreased cardiac and metabolic activity).
Stage 2 non-REM sleep is characterized by sleep spindles and K-Complexes.
A sleep spindle is a burst of oscillatory brain activity visible on an EEG that occurs specifically during stage 2 sleep. Sleep spindles are generated in the reticular nucleus of the thalamus, and may represent periods in which the brain is inhibiting processing to keep the sleeper in a tranquil state. During sleep these spindles are seen in the brain as a burst of activity immediately following muscle twitching. Spindles have been shown to aid sleeping in the presence of disruptive external sounds, and have also been associated with the integration of new information into existing knowledge, as well as with directed remembering and forgetting.
K-complexes are high-voltage events that occur more frequently in the first sleep cycles. K-complexes are thought to have two main purposes:
- to limit brain activity in response to stimuli that are not dangerous, and
- to help with sleep-based memory consolidation.

Sleep spindles and K-complexes: Sleep spindles and K-complexes are defining characteristics and indicate the onset of stage 2 NREM sleep.
2.3.1.3 – Stage 3 NREM (N3)
Stage 3 of non-REM sleep is considered the start to “deep sleep.” A sleeper first enters stage three approximately 30 to 45 minutes into sleeping. This is the stage in which different forms of parasomnia, such as night terrors, nocturnal enuresis, sleepwalking, and somniloquy (sleep talking) typically occur. This stage, formerly divided into two separate stages (3 and 4), is called slow-wave sleep, or SWS. In SWS, the sleeper is less responsive to the environment; many environmental stimuli no longer produce any reactions.
It is characterized by the following:
- Delta waves, or, very slow brain waves.
- Deeper sleep; it is much harder to wake up someone in this phase of sleep than someone in stage 1 or 2 sleep.
- If awakened during this phase, a person will likely experience disorientation and grogginess.
The sleeper will go through NREM stage 2 once again before entering REM sleep.
2.3.2 – REM Sleep
The sleeper now enters rapid eye movement (REM) sleep. In this stage, most muscles are paralyzed. This level is also referred to as paradoxical sleep because the sleeper, although exhibiting EEG waves similar to a waking state, is harder to arouse than at any other sleep stage.
REM sleep accounts for 20–25% of total sleep time in most human adults. The criteria for REM sleep include rapid eye movements as well as a rapid low-voltage EEG. During REM sleep, EEG patterns return to higher-frequency saw-tooth waves. Most memorable dreaming occurs in this stage. Partial paralysis occurs, perhaps to protect organisms from self-damage through physically acting out scenes from the often-vivid dreams that occur during this stage. Vital signs indicate arousal, and oxygen consumption by the brain is higher than when the sleeper is awake.
2.3.3 – Sleep Cycles
Sleep has four distinct phases, or stages. Sleep progresses from stage 1 to stage 2 to stage 3, and then back to stage 2 before transitioning into the REM phase. Once the REM phase is over, stage 2 will repeat. A person will complete this entire cycle about four or five times given a full night of sleep.
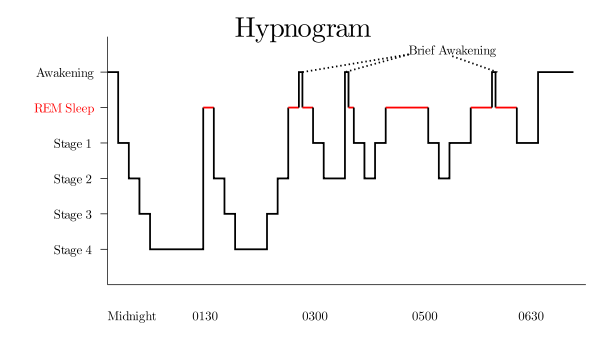
A typical night’s sleep: This sample hypnogram (EEG of sleep) shows how the proportion of the sleep cycle spent in REM sleep increases with each subsequent cycle over the course of a night. (Note that stages 3 and 4 are now considered to be one stage, stage 3.)
A sleeper first enters REM sleep after about an hour and a half of sleep, and then the phase will last only briefly. However, for each successive sleep cycle, the proportion of the cycle spent in REM sleep increases, up to an hour long in later cycles. This is why it is important for humans to sleep in long stretches (e.g., once a day for 8 hours) rather than in short bursts (e.g., 4 times a day for 2 hours each time); we spend much less total time in REM sleep than we do when we get one long period of sleep, and we can’t get through the stages we need to heal and stay healthy.
2.3.4 – Sleep Deprivation
Sleep deprivation tends to cause slower brain waves in the frontal cortex, shortened attention span, higher anxiety, impaired memory, and an unhappy mood. Conversely, a well-rested organism tends to have improved memory and mood. Research has demonstrated that some sleep stages are more important than others in achieving restfulness. For example, REM deprivation causes a significant increase in the number of attempts to go into the REM stage while asleep. On recovery nights, an individual will most likely move to stage 3 and REM sleep more quickly and experience “REM rebound,” which refers to a large increase in the time spent in the REM stage. These findings are consistent with the idea that REM sleep is biologically necessary. REM sleep is thought to be largely responsible for the time that our brains take to consolidate learning and memory. Similarly, sleeping in short bursts is not sufficient for restfulness because it does not allow our bodies enough time for a complete cycle of sleep.
2.4 – Sleep-Wake Disorders
2.4.1 – Introduction
Sleep disorders cause sleep disturbances that affect the amount, quality, or timing of sleep or that induce abnormal events during sleep.
Sleep-wake disorders cause a number of sleep disturbances that affect the amount, quality, or timing of sleep or that induce abnormal events during sleep. Some sleep-wake disorders are serious enough to interfere with normal physical, mental, and emotional functioning. Disruptions in sleep can be caused by a variety of issues, from teeth grinding (bruxism) to night terrors. Polysomnography is a technique that can be used to identify some sleep disorders.
2.4.2 – Insomnia Disorder
Insomnia refers to a chronic difficulty in falling asleep and/or maintaining sleep when no other cause is found for these symptoms. It is often a symptom of a mood disorder (e.g., emotional stress, anxiety, depression), an underlying health condition (e.g., asthma, diabetes, heart disease, pregnancy, or a neurological condition), or abuse of alcohol or drugs. However, it can also be a disorder in its own right.
The DSM-5 diagnostic criteria for insomnia disorder are as follows:
- The person experiences dissatisfaction with sleep quantity or quality as a result of difficulty initiating or maintaining sleep.
- As a result the person experiences clinically significant distress or impairment in social, occupational, educational, academic, behavioral, or other important areas of functioning.
- The sleep difficulty occurs despite adequate opportunity for sleep.
- The sleep difficulty occurs at least 3 nights per week.
- The sleep difficulty is present for at least 3 months.
The DSM-5 also provides the following exclusion criteria:
- The insomnia must not be better explained by and must not occur exclusively during the course of another sleep-wake disorder (e.g., narcolepsy, a breathing-related sleep disorder, a circadian rhythm sleep-wake disorder, a parasomnia).
- The insomnia must not be attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication).
- Coexisting mental disorders and medical conditions must not adequately explain the predominant complaint of insomnia.
2.4.3 – Hypersomnolence Disorder
Hypersomnolence disorder (also known as idiopathic hypersomnia) is a disease of likely neurological origin that is characterized primarily by severe, excessive daytime sleepiness. It has been diagnosed only rarely and is often very difficult to diagnose at an early stage. It is usually a debilitating lifelong disease. There is a very low level of public awareness of this disorder, which often results in stigmatization of those who suffer from it. Currently, there is no cure, there are no FDA-approved treatments, and research funding for the study of this disorder is scarce.
2.4.4 – Narcolepsy

Narcolepsy: Narcolepsy is characterized by an individual uncontrollably falling asleep very suddenly, typically in inappropriate situations.
Narcolepsy is also referred to as excessive daytime sleepiness (EDS). Individuals with this disorder often fall asleep spontaneously but unwillingly at inappropriate times. People with narcolepsy tend to have trouble in areas such as work, leisure, and personal relationships.
2.4.5 – Breathing-Related Sleep Disorders
Some sleep disorders are caused by disturbances in breathing. Sleep apnea, for example, is a disorder in which obstruction of the airway during sleep causes a lack of sufficient deep sleep, often accompanied by snoring.
Sleep apnea is usually caused by some sort of physical condition that obstructs the breathing system, such as obesity, rather than a mental condition. The DSM-5 names two types of sleep apnea: obstructive sleep apnea, in which your airway collapses during sleep, and central sleep apnea, in which your brain does not signal your lungs to continue to inhale.
Individuals with sleep apnea often feel tired throughout the day, as the constant breaks in their sleep cycle cause unrestful nights.
2.4.6 – Parasomnias
Parasomnias are a category of sleep disorders that involve abnormal movements, behaviors, emotions, perceptions, and dreams that occur while falling asleep, while sleeping, while between sleep stages, or during arousal from sleep. Most parasomnias are due to partial arousal during the transitions between wakefulness and non-rapid-eye-movement (N-REM) sleep or between wakefulness and rapid-eye-movement (REM) sleep.
2.4.7 – Sleepwalking (Somnambulism)
Sleepwalking (sometimes called sleepwalking disorder, somnambulism, or noctambulation) causes a person to get up and walk during the early hours of sleep. The person may sit up and look awake (though they’re actually asleep), get up and walk around, move items, or dress or undress themselves. They will have a blank stare and still be able to perform complex tasks. Some individuals also talk while in their sleep, saying meaningless words and even having arguments with people who are not there. A person who sleepwalks will be confused upon waking up and may also experience anxiety and fatigue.
Sleepwalking can be dangerous—people have been known to seriously hurt themselves during sleepwalking episodes. It is most common in children, but it also occurs occasionally in adults. For adults, alcohol, sedatives, medications, medical conditions and mental disorders are all associated with sleepwalking.
2.4.8 – Sleep Terrors and Nightmare Disorder
Sleep terrors are characterized by a sudden arousal from deep sleep with a scream or cry, accompanied by some behavioral manifestations of intense fear. Sleep terrors typically occur in the first few hours of sleep, during stage 3 NREM sleep. Night terrors tend to happen during periods of arousal from delta sleep (i.e., slow-wave sleep). They are worse than nightmares, causing significant disorientation, panic, and anxiety. They can last up to 10 minutes, and the person may be screaming and difficult to wake. In adults, it is often a symptom of some psychopathology.
Distinct from sleep terrors is nightmare disorder. Also known as “dream anxiety disorder,” nightmare disorder is characterized by frequent nightmares. The nightmares, which often portray the individual in a situation that jeopardizes their life or personal safety, usually occur during the second half of the sleeping process, called the REM stage. Though many people experience nightmares, those with nightmare disorder experience them more frequently.
2.4.9 – Restless Legs Syndrome
Restless legs syndrome (RLS) is a neurological disorder characterized by an irresistible urge to move one’s body to stop uncomfortable or odd sensations. It most commonly affects the legs, but it can also affect the arms, torso, head, and even phantom limbs. Moving the affected body part modulates the sensations, providing temporary relief. RLS may start at any age, including childhood. For some it is a progressive disease; for others the symptoms decrease over time.
2.5 – The Nature and Meaning of Dreams
2.5.1 – Introduction
Numerous theories, both psychological and neurobiological, have been proposed to explain the elusive mystery of the purpose of dreaming.

The long-standing mystery of dreams: Since ancient times, humans have been trying to understand the purpose of dreams.
For centuries people have pondered the meaning of dreams. Early civilizations thought of dreams as a medium between our earthly world and that of the gods. In fact, the Greeks and Romans were convinced that dreams had certain prophetic powers. Over the years, numerous theories have been put forth in an attempt to illuminate the mystery behind human dreams. Only recently has strong, tangible evidence become less elusive.
2.5.2 – Psychological Theories of Dreaming
2.5.2.1 – Freudian and Jungian Theories
While there has always been great interest in the interpretation of human dreams, it was not until the end of the nineteenth century that Sigmund Freud and Carl Jung put forth some of the most widely-known modern theories of dreaming. Freud’s theory centered around the notion of repressed longing or wish fulfillment—the idea that dreaming allows us to sort through unresolved, repressed wishes. Freud’s theory described dreams as having both latent and manifest content. Latent content consists of deep unconscious wishes or fantasies, while manifest content is superficial and meaningless. Manifest content often masks or obscures latent content. It was in his book The Interpretation of Dreams (published in 1900) that Freud first argued that the motivation of all dream content is wish-fulfillment, and that the instigation of a dream is often to be found in the events of the day preceding the dream, which he called the “day residue.” Later, Freud revised his theory to suggest that dreams may also represent the repetition compulsion, which is a psychological phenomenon in which a person repeats a traumatic event or its circumstances over and over again. This can take the form of reenacting the event—which can include “reliving” the scenario in the form of dreams—or putting oneself in situations where the event is likely to happen again.
Carl Jung (who studied under Freud) also believed that dreams had psychological importance, but proposed different theories about their meaning. Jung expanded on Freud’s idea that dream content relates to the dreamer’s unconscious desires. He thought of dreams as messages to the dreamer, containing revelations that could uncover and possibly resolve emotional or religious problems and fears.
2.5.2.2 – Threat Simulation Theory
Threat-simulation theory suggests that dreaming should be seen as an ancient biological defense mechanism. Dreams are thought to provide an evolutionary advantage because of their capacity to repeatedly simulate potential threatening events. This process enhances the neurocognitive mechanisms required for efficient threat perception and avoidance.
During much of human evolution, physical and interpersonal threats were serious enough to reward reproductive advantage to those who survived them. Therefore, dreaming evolved to replicate these threats and allow people to regularly practice dealing with them. This theory suggests that dreams serve the purpose of allowing for the rehearsal of threatening scenarios in order to better prepare an individual for real-life threats.
2.5.2.3 – Expectation-Fulfillment Theory
This theory posits that dreaming serves to discharge emotional arousals (however minor) that haven’t been expressed during the day. This practice frees up space in the brain to deal with the emotional arousals of the next day and allows instinctive urges to stay intact. In effect, the expectation is fulfilled (the action is “completed”) in a metaphorical form so that a false memory is not created. This theory explains why dreams are usually forgotten immediately afterwards.
2.5.3 – Neurobiological Theories
2.5.3.1 – Activation-Synthesis Theory
One prominent neurobiological theory of dreaming is the activation-synthesis theory, which states that dreams don’t actually mean anything. They are merely electrical brain impulses that pull random thoughts and imagery from our memories. The theory posits that humans construct dream stories after they wake up, in a natural attempt to make sense of the nonsensical. However, given the vast documentation of the realistic aspects of human dreaming, as well as indirect experimental evidence that other mammals such as cats also dream, evolutionary psychologists have theorized that dreaming does indeed serve a purpose.
2.5.3.2 – Continual-Activation Theory
The continual-activation theory proposes that dreaming is a result of brain activation and synthesis. Dreaming and REM sleep are simultaneously controlled by different brain mechanisms. The hypothesis states that the function of sleep is to process, encode, and transfer data from short-term memory to long-term memory through a process called consolidation. However, there is not much evidence to back this up. NREM sleep processes the conscious-related memory (declarative memory), and REM sleep processes the unconscious related memory (procedural memory).
The underlying assumption of continual-activation theory is that, during REM sleep, the unconscious part of the brain is busy processing procedural memory. Meanwhile, the level of activation in the conscious part of the brain descends to a very low level as the inputs from the senses are basically disconnected. This triggers the “continual-activation” mechanism to generate a data stream from the memory stores to flow through to the conscious part of the brain.
3 – Altered States of Consciousness
3.1 – Dissociation
Dissociation is the experience of feeling detached from reality.
3.1.1 – The Continuum of Dissociatin
In psychology, the term “dissociation” describes a wide array of experiences, from mild detachment from immediate surroundings to more severe detachment from physical and emotional experience. The major characteristic of all dissociative phenomena involves a detachment from reality. Although some dissociative experiences involve memory loss, others do not.
Dissociative experiences can be placed on a continuum from non-pathological to pathological, where pathological means “caused by a mental disorder.” At the non-pathological end of the spectrum, the term “dissociation” can be used to describe events as common as daydreaming during class. Further along the continuum are altered states of consciousness which can lead to dissociation. At the pathological end of the dissociation spectrum are the dissociative disorders.
3.1.2 – Non-Pathological Dissociation
3.1.2.1 – Daydreaming

Daydream by Paul César Helleu: Daydreaming is a mild form of dissociation in which a person experiences a short-term detachment from one’s immediate surroundings.
Daydreaming, experienced while awake, is a short-term detachment from one’s immediate surroundings, during which a person’s contact with reality is blurred and partially substituted by a visionary fantasy, especially one of happy, pleasant thoughts, hopes, or ambitions imagined as coming to pass.
There are many types of daydreams, and there is no consistent definition among psychologists, but all daydreaming meets the criteria for mild dissociation.
3.1.2.2 – Coping
Coping is expending conscious effort to solve personal and interpersonal problems, and seeking to minimize or tolerate stress or conflict. Psychological coping mechanisms are commonly called coping strategies or coping skills. In mild instances, dissociation is regarded as a coping mechanism designed to master, minimize, or tolerate stressors like boredom or conflict. Coping through dissociation is often associated with post-traumatic stress syndrome.
3.1.2.3 – Altered States
Psychoactive drugs can often induce a state of temporary dissociation. Substances with dissociative properties include ketamine, nitrous oxide, alcohol, LSD, tiletamine, marijuana, dextromethorphan, PCP, methoxetamine, salvia, and muscimol.
3.1.3 – Pathological Dissociation
Pathological dissociation involves the dissociative disorders, including dissociative fugue and depersonalization disorder. Dissociative disorders are sometimes triggered by trauma, but may be preceded only by stress, psychoactive substances, or no identifiable trigger at all. The Diagnostic and Statistical Manual of Mental Disorders groups all dissociative disorders into a single category.
Dissociative disorders are typically experienced as startling, autonomous intrusions into a person’s usual ways of responding or functioning. Due to their unexpected and largely inexplicable nature, they tend to be quite unsettling.
Dissociation has been described as one of a constellation of symptoms experienced by some victims of childhood trauma, including physical, psychological, and sexual abuse. This is supported by studies which suggest that dissociation is correlated with a history of trauma. Dissociation is much more common among those who are traumatized (this is called “high specificity” to history of trauma), but at the same time there are many people who have suffered from trauma but who do not show dissociative symptoms (this is called “low sensitivity” to history of trauma).
3.2 – Meditation
3.2.1 – Introduction

Meditation: Meditation allows a person to achieve a mental and physical state of relaxation.
Meditation is the practice of training the mind in order to induce relaxation or an altered mode of consciousness.
Meditation is the practice of training the mind to think in a particular way or to induce some mode of consciousness. This is done to obtain a particular benefit, such as relaxation, or as an end in itself. Meditation encompasses a variety of techniques that help a person achieve relaxation, build internal energy, or develop compassion and patience. Techniques of meditation vary from person to person and from culture to culture.
Daily meditation can be helpful for a variety of reasons. Western studies are beginning to show what other cultures have known for centuries—namely, that meditation helps to reduce stress, assists individuals in gaining perspective, enhances focus, and contributes to physical and psychological health and well-being. Meditation can be done any time of the day, and it can take as few as five minutes or as long as several hours.
3.2.2 – Techniques and Varieties of Meditation
Different meditation techniques include meditation of breath, devotional meditation, and relaxation meditation. Meditation of breath can be described as the most traditional form of meditation, in which a person sits comfortably and focuses on his or her breath entering and leaving the body. The concentration involved in this type of meditation helps clear a person’s mind and allows him or her to enter a state of deep relaxation and clear mind.
Devotional meditation is very similar to meditation of breath, except instead of focusing on the breath entering and leaving a person’s body, the focus is on a particular object or concept. Many ancient religions of the world have a tradition of using some type of prayer beads as tools in devotional meditation. The object chosen assists the individual in focusing and calming his or her mind, often through repeated movements. Meditation may also involve repeating a mantra and closing one’s eyes.
Relaxation meditation, also known as progressive muscle relaxation, allows a person to fully relax his or her entire body. This kind of relaxation involves systematically and rhythmically tightening and relaxing various muscle groups. By tightening and relaxing the various muscle groups in a person’s body, often working from one end of the body to another, relaxation (both physical and mental) is achieved.
3.2.3 – Health Benefits of Meditation
There are a variety of health benefits associated with meditation, and research continues to show more evidence of these benefits in studies involving meditation. Though this is not an exhaustive list, some of the health benefits include the following:
- increased blood flow to all parts of the body;
- lower blood pressure;
- reduced anxiety;
- decreased muscle tension;
- lower rates of depression due to increased serotonin levels;
- enhanced immune system.
3.2.4 – Research on Meditation
Research on the effects of meditation is a growing subfield of neurological research. Modern scientific techniques and brain-scan instruments have been used to see what happens in the bodies of people when they meditate, and how their bodies and brains change after meditating regularly.
Studies have shown that rumination and worry contribute to mental illnesses such as depression and anxiety, and that meditation-based interventions are effective in the reduction of worry, even in such extreme cases as panic disorder and post-traumatic stress disorder (PTSD). These interventions also appear to bring about favorable structural changes in the brain. A recent study found a significant cortical thickness increase in individuals who underwent a brief eight-week training program, and that this increase was coupled with a significant reduction of several psychological indices related to worry, anxiety, and depression. Another study describes how meditation-based interventions target neurocognitive mechanisms of addiction.
3.3 – Hypnosis
3.3.1 – Introduction
Hypnosis is a trance-like state in which a person experiences heightened suggestibility. When a person is in this altered state of perception, it is thought that he or she can be guided to experience a reduction in pain, alter ineffective cognitions or beliefs, or remember forgotten memories, among other things.
3.3.2 – Theories of Hypnosis
Three main theories of hypnosis exist:
- Role theory is when a person is not actually in an alternate state of consciousness, but rather is acting out the role of a hypnotized person.
- Altered-state theory occurs when a person is actually hypnotized and is therefore in a different, or altered, state of mind.
- Dissociation theory states that hypnosis causes a person to actively or voluntarily split their consciousness.
Controversy exists regarding which of these theories is true, and research has yet to illuminate exactly what occurs in hypnosis, or how.
3.3.3 – Components of Hypnosis
There are three main components of hypnosis:
- Absorption is the amount of investment a person has in the hypnotic state or hypnosis session. Generally speaking, the more suggestible a person is, the more he or she can dissociate and become absorbed in the task at hand. This is known as mental concentration.
- Dissociation is when a person’s behavioral control is separated from his or her awareness. The individual in a dissociated state is likely to respond with autonomic, reflexive behaviors.
- Suggestion is the act of focusing the conscious mind on a single idea. A point person (usually the psychologist/hypnotist) guides the hypnotized person’s thoughts, feelings, or behaviors, helping the person change ideas of their choice. It is important to note that suggestion is not the same thing as trance. A trance is when an induced mental state facilitates the acceptance of instructions or ideas.
3.3.4 – Uses of Hypnosis
Hypnotic colors: The use of colorful images can help people relax into a hypnotic state.
Hypnosis serves many purposes. It can be used for pain management when traditional methods do not seem to be working. For example, some women engage in what is known as hypnobirthing, thereby reducing the need for pain medication during labor.
The use of hypnotism for therapeutic purposes is referred to as hypnotherapy, while its use as a form of entertainment for an audience is known as stage hypnosis. Hypnotherapy has been used to address addiction, weight loss, fears and phobias, and to release repressed memories, which may have given rise to negative effects. Hypnosis has also been used to treat physical ailments such as irritable bowel syndrome and psoriasis, and it has been successfully used in the treatment of post-traumatic stress disorder, depression, and anxiety.
4 – How Psychoactive Drugs Impact the Brain
4.1 – Depressants
4.1.1 – Introduction
Depressants cause the body to relax by increasing the neurotransmitter GABA, which decreases neuronal excitability.
A depressant (also called a central depressant) is a chemical compound that manipulates neurotransmission levels, thereby reducing arousal or stimulation in various parts of the brain. Depressants are also occasionally referred to as “downers” because they lower the level of arousal in the brain when taken. Stimulants, or “uppers,” which increase mental and/or physical function, are the functional opposites of depressants.
4.1.2 – Effects of Depressants
Depressants are widely used throughout the world as prescription medicines and as illicit substances. Effects often include ataxia, anxiolysis, pain relief, sedation or somnolence, and cognitive/memory impairment; in some instances, effects include euphoria, dissociation, muscle relaxation, lowered blood pressure or heart rate, respiratory depression, anticonvulsant effects, and even complete anesthesia or death. Calming effects of depressants may be beneficial to those suffering from anxiety, sleep disorders, or pain; however, the more extreme effects can be dangerous and even life-threatening.
On the neural level, most depressants act on the brain by affecting the neurotransmitter gamma-aminobutyric acid (GABA), which is responsible for regulating (specifically, decreasing) neuronal excitability throughout the nervous system.
Neurotransmitters are brain chemicals that facilitate communication between brain cells. Depressants inhibit the next neuron from sending impulses by binding to receptor molecules. Although the different classes of depressants work in unique ways, it is through their ability to increase GABA—and thereby inhibit brain activity—that they produce a drowsy or calming effect.
4.1.3 – Types of Depressants
4.1.3.1 – Alcohol

Alcohol as a depressant: Alcohol depresses the brain, resulting in relaxation and impaired judgment.
Barbiturates are effective as anxiolytics, hypnotics, and anticonvulsants, and also have an analgesic (painkiller) effect. However, they are commonly misused, physically addictive, and have serious potential for overdose. In the late 1950s, it became clear that the social cost of barbiturates was beginning to outweigh the medical benefits, which sparked a serious search for a class of replacement drugs. Most people still using barbiturates today do so to prevent seizures or for relief of migraine symptoms.
Barbiturates have been largely replaced by benzodiazepines, because the latter have fewer side effects and less potential for lethal overdoses. However, barbiturates are still used as anti-convulsants (e.g., phenobarbital, an anti-seizure medication), as sedatives (e.g., sodium thiopental), and analgesics for cluster headaches and migraines (e.g., Fioricet).
4.1.3.2 – Barbiturates
Barbiturates are effective as anxiolytics, hypnotics, and anticonvulsants, and also have an analgesic (painkiller) effect. However, they are commonly misused, physically addictive, and have serious potential for overdose. In the late 1950s, it became clear that the social cost of barbiturates was beginning to outweigh the medical benefits, which sparked a serious search for a class of replacement drugs. Most people still using barbiturates today do so to prevent seizures or for relief of migraine symptoms.
Barbiturates have been largely replaced by benzodiazepines, because the latter have fewer side effects and less potential for lethal overdoses. However, barbiturates are still used as anti-convulsants (e.g., phenobarbital, an anti-seizure medication), as sedatives (e.g., sodium thiopental), and analgesics for cluster headaches and migraines (e.g., Fioricet).
4.1.3.3 – Benzodiazepines
Benzodiazepines enhance the effect of the neurotransmitter gamma-aminobutyric acid (GABA) at the GABA receptor, resulting in sedative, hypnotic (sleep-inducing), anxiolytic (anti-anxiety), anticonvulsant, and muscle-relaxant properties. Amnesic-dissociative actions are also seen in the applied pharmacology of high doses of many shorter-acting benzodiazepines. These properties make benzodiazepines useful in treating anxiety, insomnia, agitation, seizures, muscle spasms, alcohol withdrawal, and as a premedication for medical or dental procedures. Some of the most common benzodiazepines are anti-anxiety medications, such as clonazepam (Klonopin), alprazolam (Xanax), diazepam (Valium), and zolpidem (Ambien).
4.1.3.4 – Cannabinoids
Although cannabis or marijuana is often considered either in its own unique category or as a mild psychedelic, the drug—notably the chemical compound cannabidiol that it contains—nevertheless has many depressant effects such as muscle relaxation, sedation, decreased alertness, and tiredness. There are at least 85 different cannabinoids isolated from cannabis, the most common of which is THC, the active ingredient in marijuana. Cannabinoids can be administered by smoking, vaporizing, oral ingestion, transdermal patch, intravenous injection, sublingual absorption, or rectal suppository. Once in the body, most cannabinoids are metabolized in the liver.
4.1.3.5 – Opioids
An opioid is any psychoactive chemical that resembles morphine or other opiates in its pharmacological effects. One of the oldest known drugs, opioids induce an analgesic (painkiller) effect by decreasing perception of pain, decreasing reaction to pain, and increasing pain tolerance. Known for their highly addictive quality, opioids work by binding to opioid receptors, which are found principally in the central and peripheral nervous system and the gastrointestinal tract. Opioids are among the world’s oldest known drugs; therapeutic use of the opium poppy predates recorded history. The most common opioids in modern history are morphine, heroin, and codeine, which are known as incredibly effective, albeit addictive, painkillers. As opposed to these naturally occurring opioids that are derived directly from the resin of the poppy plant, synthetic opioids are synthesized chemically in the laboratory and are agents commonly used in pain relief, treating drug dependence and anesthesia. Some examples include hydrocodone and oxycodone.
4.1.3.6 – A Note on the Term “Narcotics”
The term “narcotic” originally referred medically to any psychoactive compound with sleep-inducing properties. In the United States, it has since become associated with opioids, commonly morphine and heroin and their derivatives. The term is, today, imprecisely defined and typically has negative connotations. When used in a legal context in the United States, the term “narcotic drug” refers to a substance that is completely prohibited, or one, such as codeine or morphine, that is used in violation of governmental regulation. From a medical standpoint, it is no longer a useful term.
4.2 – Stimulants
Stimulants induce temporary improvements in mental and/or physical functions and are commonly used as prescription or recreational drugs.
4.2.1 – Function of Stimulants
Stimulants are psychoactive drugs that induce temporary improvements in mental and/or physical functions. Occasionally referred to as “uppers,” stimulants are the functional opposites of depressants, or “downers,” which decrease mental and/or physical function. Stimulants are widely used throughout the world as prescription medicines and as illicit substances of recreational use or abuse.
Stimulants increase the activity of the central nervous system (the brain and spinal cord), the sympathetic nervous system (part of the peripheral nervous system that controls the fight-or-flight response), or both. Common effects, which vary depending on the substance in question, may include enhanced alertness, awareness, wakefulness, endurance, productivity, and motivation. Effects can also include an increase in arousal, locomotion, heart rate, and blood pressure, and the perception of diminished requirements for food and sleep. Some stimulants produce a sense of euphoria, especially those that exert influence on the central nervous system.
4.2.2 – Neurological Mechanism of Stimulants
Stimulants exert their effects through a number of different mechanisms. Some stimulants facilitate the activity of certain neurotransmitters, specifically norepinephrine and/or dopamine. Others block the action of certain receptors (such as the adenosine receptors) in a process known as receptor antagonism. Still others cause action in other receptors (such as nicotinic acetylcholine) in a process known as receptor agonism.
4.2.3 – Use and Abuse of Stimulants
Therapeutically, stimulants are used and/or prescribed for a variety of reasons. They are used to increase or maintain alertness; to boost endurance or productivity; to counteract fatigue and lethargy throughout the day; to counteract abnormal states that diminish alertness or consciousness (such as in narcolepsy); to decrease appetite and promote weight loss; and to enhance concentration (especially for those with attentional disorders such as ADHD). Many stimulants are also capable of improving mood and relieving anxiety, and are occasionally used to treat symptoms of depression.
The euphoria produced by some stimulants leads to their recreational use, so many stimulants are either illegal or very carefully controlled in the United States. Some may be legally available only by prescription. Addiction to some central-nervous-system stimulants can quickly lead to medical, psychiatric, and psychosocial deterioration. Drug tolerance, dependence, sensitization, and withdrawal can occur after repeated use. Over time, stimulants can disrupt the functioning of the brain’s dopamine system, dampening users’ ability to feel any pleasure at all.
4.2.4 – Types of Stimulants
Examples of well-known stimulants include amphetamines, MDMA, NDRIs, cocaine, caffeine, and nicotine.
4.2.4.1 – Amphetamines
Amphetamines (such as ephedrine and methamphetamine) are a group of stimulants that increase the levels of norepinephrine and dopamine in the brain through reuptake inhibition—meaning they block these neurotransmitters from being reabsorbed back into the neural networks. Amphetamines are known to cause elevated mood and euphoria, and are often used for their therapeutic effects. Physicians occasionally prescribe amphetamines to treat major depression, and numerous studies have demonstrated the effectiveness of drugs such as Adderall in controlling symptoms associated with ADHD. Due to their availability and fast-acting effects, amphetamines are prime candidates for abuse.
4.2.4.2 – MDMA
Methylenedioxymethamphetamine (MDMA), known by its common street names Ecstasy and Molly, had a medical application as a treatment for depression and a psychotherapy aid until 1985, when it became a controlled substance. The stimulant effects of MDMA include appetite loss, euphoria, social disinhibition, insomnia, improved energy, increased arousal, and increased perspiration.
MDMA also has many physical side effects: since MDMA increases the activity of serotonin, the brain becomes depleted of serotonin, causing a rebound sadness or depression in the days following use. MDMA differs from most stimulants in that its primary pharmacological effect is on the neurotransmitter serotonin rather than dopamine, epinephrine, or norepinephrine. MDMA also decreases the release of dopamine. The increase in seratonin is caused because the MDMA prevents seratonin from entering the reuptake site, causing a continued flow, and eventually excess seratonin.
4.2.4.3 – NDRIs
Norepinephrine and dopamine reuptake inhibitors (NDRIs) (such as the antidepressant Wellbutrin) inhibit the uptake of dopamine and norepinephrine, effectively increasing their amounts in the brain and causing a stimulating effect. Many of these compounds are effective ADHD medications and antidepressants. These medicines have an extended release mechanism, and are typically less popular for recreational use.
4.2.4.4 – Cocaine

Cocaine: Cocaine, in powder form, is a commonly abused stimulant that produces a sense of euphoria in the user.
Cocaine is made from the leaves of the coca shrub, which grows in the mountain regions of South America. In Europe and North America, the most common form of cocaine is a white crystalline powder. Most cocaine use is recreational and its abuse potential is high, and so its sale and possession are strictly controlled in most jurisdictions.
4.2.4.5 – Caffeine and Nicotine
Caffeine is a drug that is found naturally in coffee, tea, soft drinks, and cocoa. Caffeine stimulates the body, increases heart rate and blood pressure, and facilitates alertness and concentration. The vast majority (over 80%) of people in the United States consume caffeine on a daily basis. In very low concentrations, nicotine also acts as a stimulant, and it is one of the main factors responsible for the dependence-forming properties of tobacco.
4.3 – Hallucinogens
4.3.1 – Introduction
Hallucinogens affect the levels of serotonin or glutamate in the brain and are divided into psychedelics, dissociatives, and deleriants.

Naturally occuring hallucinogen: Hallucinogenic mushrooms often have a characteristic blue bruising on their stems.
Hallucinogens are drugs that alter sensory input to the brain. This creates an altered sense of reality, as well as a change in emotions and thought patterns. Hallucinogens can connect the conscious mind to the unconscious, delivering thoughts and feelings that would otherwise remain out of our conscious awareness.
Hallucinogens are divided into three categories: psychedelics, dissociatives, and deliriants.
4.3.2 – Psychedelics
Psychedelics are distinguished from the other two subclasses by their lack of addictive qualities, as well as the remarkable experiences one may have under their influence. Most (but not all) psychedelics are non-toxic and have a very high LD50. This means that the user would have to ingest or take very large amounts of the drug, many times that of a recreational dose, in order to kill themselves. The resulting experiences, however, can be extremely overwhelming, often driving users to seek emergency assistance.
4.3.3.1 – Effect of Psychedelics on the Brain
Most psychedelics work by interacting with serotonin receptors in the brain. Effects include increased breathing and heart rate, dilated pupils, dehydration, increased color perception, a state of empathetic well-being (feeling as though one is at peace with everyone and everything), and visual distortion: things may appear to move, shapes may appear on textures and exhibit a kaleidoscope-like effect, or lighting may dramatically change for no apparent reason.
4.3.4 – Dissociatives
Dissociatives are a subclass of hallucinogens that work by blocking or altering sensory perception (including senses that are perceived by the unconscious mind), creating a feeling of disconnection and depersonalization from one’s body and reality in general. Many dissociatives are strong depressants, and large doses can slow down the heart or breathing to the point of causing death. Generally they are not physically addictive, but can be habit forming if used repeatedly in a short time span.
4.3.4.1 – Effect of Dissociatives on the Brain
Most dissociative drugs simulate a dream-like experience. As with psychedelics, a mixing of the senses can lead users to believe they can see sounds or taste textures. Primary dissociatives are NMDA antagonists, which block glutamate from entering its receptors and regulating brain function.
4.3.5 – Deliriants
Deliriants are very similar to dissociatives, and are considered to be true hallucinogens because the visuals they produce are hard or impossible to distinguish from reality. Under their influence, users will often have entire, rational conversations with people who aren’t actually there. Some people may see their own reflection and believe it is another person copying their actions. Users often retain awareness of their physical surroundings, but are consciously impaired. Almost all deliriants are toxic enough that there is a very small difference, in terms of quantity used, between a recreational dose and a lethal one. Both Benadryl and Dramamine are deliriants when taken in extremely high quantities.
4.3.5.1 – Effect of Deliriants on the Brain
Deliriants work by inhibiting acetylcholine, a neurotransmitter responsible for cognition and stimulation. By contrast, when you drink a cup of coffee, your acetylcholine increases, leading to enhanced alertness and focus.
4.3.6 – Common Hallucinogens
4.3.6.1 – Psychedelics
Psilocybin mushrooms, also known as “shrooms,” are mushrooms that contain the psychedelic compounds psilocybin and psilocin. They are mainly used as recreational drugs, whose effects include euphoria, altered thinking processes, closed- and open-eye visuals, synesthesia, an altered sense of time, and spiritual experiences.
LSD, also a psychedelic, blocks serotonin from the brain, which regulates mood, perception, muscle contraction, and other cognitive functions. LSD blocks serotonin because it is, structurally, similar to serotonin. For this reason, the brain mistakes LSD for serotonin and directs it to the synaptic cleft (instead of actual serotonin). LSD causes a number of alterations in perception by affecting both cognitive and visual sensory systems, and it changes the sense of time, body-image, and ego. Memory is also greatly affected. A typical “trip” can last anywhere between six and ten hours.
4.3.6.2 – Dissociatives
PCP (or angel dust), a dissociative, prevents the actions normally caused when a neurotransmitter called glutamate is able to attach to its receptor in the brain. It also disrupts the actions of other neurotransmitters. This drug is addictive, and its effects are very unpredictable. For example, it may make some people hallucinate and become aggressive, while others may become drowsy and passive.
Dextromethorphan is the active ingredient in most over-the-counter and prescription cough medicines. When used in excess of specified maximum dosages, dextromethorphan acts as a dissociative. It can produce effects similar to the dissociative states created by other dissociative anaesthetics such as ketamine and phencyclidine.
Nitrous oxide, commonly known as laughing gas, is used in surgery and dentistry for its anaesthetic and analgesic effects. It is known as laughing gas due to the euphoric effects of inhaling it, a property that has led to its recreational use as a dissociative hallucinogen.
4.3.6.3 – Deliriants
While deliriants are often naturally occuring (in plant species), synthetic compounds such asdiphenhydramine (Benadryl) and dimenhydrinate (Dramamine) are also deliriants. Uncured tobacco is also a deliriant due to its very high nicotine content, resulting in a delirious hallucinogenic intoxication. Despite the fully legal status of several common deliriant plants, deliriants are largely unpopular as recreational drugs because of their unfavorable effects.
Originally published by Lumen Learning – Boundless Psychology under a Creative Commons Attribution-ShareAlike 3.0 Unported license.






